Introduction: Androgenetic alopecia, commonly known as pattern hair loss, represents a prevalent condition affecting both men and women. It is characterized by progressive hair thinning and loss in a patterned distribution. The pathophysiological mechanisms underlying androgenetic alopecia involve a complex interplay between genetic predisposition, hormonal influences, and environmental factors. This article delves into the detailed pathology of androgenetic alopecia.
Histopathological Examination: To comprehend the microscopic alterations in androgenetic alopecia affected hair follicles, a punch biopsy is taken from the affected scalp. Punch biopsies are not normally done for the diagnosis of androgenetic alopecia, but they are done as part of research and many studies have been published that involve looking at the changes in hair follicles as androgenetic alopecia develops. The punch biopsy procedure involves the extraction of a small cylindrical skin sample, encompassing the hair follicles, using a sharp instrument. The punch biopsy tool is basically a razor blade in a cylinder form instead of flat blade, attached to a handle. The punch biopsy tool is pushed into the scalp skin, taking care to angle the insertion alongside the length of the hair follicles to avoid cutting through them. The biopsy is pulled out with some tweezers and some surgical scissors may be used to cut the punch biopsy below the level of the hair follicle bulbs. The extracted tissue is then processed and examined under a microscope in a histopathology laboratory.
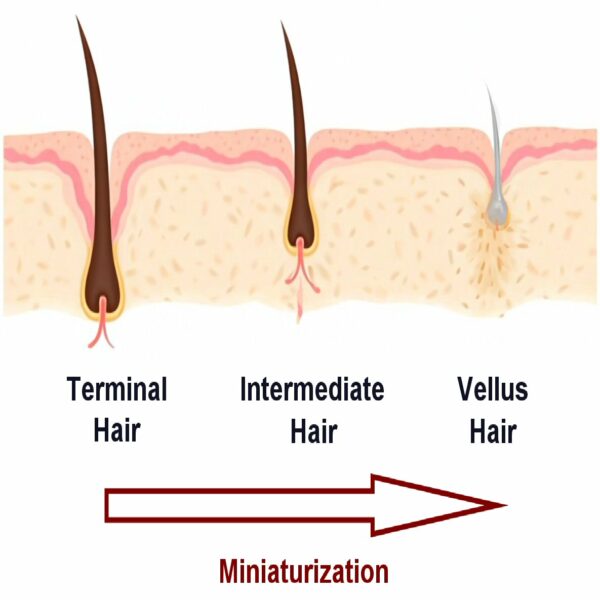
Follicular Changes: The hallmark of androgenetic alopecia is the gradual miniaturization in the size of scalp hair follicles. This occurs in both men and women with male pattern hair loss and female pattern hair loss respectively. Microscopic examination of punch biopsies from affected people often reveals a spectrum of hair follicle sizes, ranging from normal terminal hairs to significantly reduced vellus-like follicles. Terminal hairs are thick and pigmented with hair follicle bulbs up to 8mm deep below the skin surface. With pattern hair loss, these terminal follicles gradually transform into thinner, shorter, hair follicles that correspondingly make thinner, shorter and less pigmented hair fibers (often called intermediate hairs). As time continues on, these follicles continue to miniaturize into vellus-like hair follicles that make non-pigmented vellus hairs. This transition results in a visible decrease in the density of terminal hairs and an increase in vellus hairs, altering the hair follicle ratio on the scalp. For men (but usually not for women) there is one further step. The vellus follicles may degenerate and disappear completely such that even vellus hairs are no longer present. This stage of complete hair follicle destruction can take 20 years and more to complete.
Hair Cycle Alterations: In the early stages of androgenetic alopecia (usually in the first 5-10 years or so) the hair follicles may remain terminal or intermediate sized, but the condition is characterized by changes in the hair growth cycle. Normally, hair undergoes three phases: anagen (growth), catagen (regression), and telogen (resting), before returning to a full anagen growth phase again. Anagen in scalp follicles can last 5-7 years for most people – though some people have much longer anagen growth phases. In androgenetic alopecia affected individuals, there is a progressive shortening of the anagen phase, while the durations of catagen and telogen phases remain relatively unchanged. Consequently, a higher proportion of hair follicles enter the telogen phase prematurely, leading to increased hair shedding and a higher count of resting hair follicles. In unaffected scalp the percentage of hair follicles in telogen is up to 10%. In the early stages of androgenetic alopecia affected scalp the number of telogen stage hair follicles can be up to 20% of the total. With more time, the telogen phase starts to prolong. This leads to a situation where old hair fibers can be shed, but the follicle does not enter a new anagen growth phase. This results in a hair follicle in a telogen resting phase that does not contain any hair fiber – a state called “kenogen”. As time goes on, the follicles miniaturize and gradually move to a hair cycle typical of a vellus hair follicle.
Follicular Miniaturization and Fibrosis: The miniaturization process involves the shrinkage of terminal hair follicles, both in length and diameter, transitioning towards a vellus-like state. This is often accompanied by an upward migration of the hair bulb in the dermal layer. Associated with this miniaturization is the development of a fibrous streamer, or follicular stela, underneath the bulb of the miniaturizing hair follicle which marks the original position of the hair bulb. Over time, fibrosis (essentially scar tissue formation) can occur around these miniaturized follicles, further disrupting hair growth. In a punch biopsy from the scalp of a pattern hair loss affected individual, these changes and increased fibrosis can be seen using special stains for collagen deposition.
Inflammatory Response: In androgenetic alopecia, there is often an observable inflammatory infiltrate surrounding the miniaturized hair follicles, particularly in the upper dermal region. This inflammatory response is typically more pronounced than in normal scalp conditions and involves a higher density of immune cells. While mild inflammation can be seen in unaffected hair follicles, the intensity and cellularity of the inflammation are significantly increased in the presence of androgenetic alopecia. Usually this inflammation is only seen as the follicle is in the process of miniaturizing. Once the follicles reach their vellus size, the inflammation generally disappears. There are some conflicting data from different studies concerning just how common inflammation is and how significant it may be in actively promoting hair follicle miniaturization.
Hormonal Influences: Androgens, particularly dihydrotestosterone (DHT), play a crucial role in the pathogenesis of androgenetic alopecia. DHT binds to androgen receptors on hair follicle cells, leading to altered gene expression and subsequent follicular miniaturization. The sensitivity of hair follicles to androgens is genetically determined, which explains the variable patterned nature of hair loss observed in this condition. Using special stains based on antibodies, it is possible to see where androgen receptors are located in air follicles. While keratinocytes do have some androgen receptors, the main expression seems to be on the dermal papilla and lower dermal sheath cells in hair follicles. Other research has shown that, as androgen receptors engage with DHT, the dermal papilla cells receive an internal signal that pushes them into senescence (basically premature old age). As time goes on and the dermal papilla cells continue to receive signals from DHT binding to their androgen receptors, the cells start to die off. Consequently, the size of the dermal papilla gets smaller as it contains fewer cells. Research has shown that the size of the dermal papilla is directly proportional to the size of hair fiber a hair follicle is able to produce. This makes sense as the dermal papilla cells in healthy terminal hair follicles send out signals to keratinocyte cells that control the size and shape of the hair fiber and also how long anagen lasts. A smaller dermal papilla means the keratinocyte cells receive a weaker signal and less stimulation to make a hair fiber. With less stimulation, the keratinocytes slow down and switch off, the hair fiber they make becomes thinner, and can grow more slowly.
Conclusion: The pathology of androgenetic alopecia is multifaceted, hormonal, genetic, and environmental components. The interplay between these influences controls hormonal signalling in hair follicles. In turn signals from androgens affect the size and shape of hair follicles and how androgenetic alopecia develops. Using a punch biopsy, scientists and dermatologists can see how the hair follicles are affected in the scalp skin. The condition is characterized by follicular miniaturization, altered hair growth cycles, and an inflammatory response. Understanding these pathophysiological aspects is crucial for developing targeted therapeutic strategies and managing this common dermatological condition effectively. Future research in this field may uncover new insights into the molecular mechanisms driving androgenetic alopecia, leading to more effective treatments and management approaches.
Kligman AM. The comparative histopathology of male-pattern baldness and senescent baldness. Clin Dermatol. 1988;6(4):108–18.
1.
Whiting DA. Diagnostic and predictive value of horizontal sections of scalp biopsy specimens in male pattern androgenetic alopecia. J Am Acad Dermatol. 1993 May;28(5 Pt 1):755–63.
1.
de Lacharrière O, Deloche C, Misciali C, Piraccini BM, Vincenzi C, Bastien P, et al. Hair diameter diversity: a clinical sign reflecting the follicle miniaturization. Arch Dermatol. 2001 May;137(5):641–6.
1.
Deloche C, de Lacharrière O, Misciali C, Piraccini BM, Vincenzi C, Bastien P, et al. Histological features of peripilar signs associated with androgenetic alopecia. Arch Dermatol Res. 2004 Mar;295(10):422–8.
1.
El-Domyati M, Attia S, Saleh F, Abdel-Wahab H. Androgenetic alopecia in males: a histopathological and ultrastructural study. J Cosmet Dermatol. 2009 June;8(2):83–91.
1.
Aslani FS, Dastgheib L, Banihashemi BM. Hair counts in scalp biopsy of males and females with androgenetic alopecia compared with normal subjects. J Cutan Pathol. 2009 July;36(7):734–9.
Torkamani N, Rufaut NW, Jones L, Sinclair R. Destruction of the arrector pili muscle and fat infiltration in androgenic alopecia. Br J Dermatol. 2014 June;170(6):1291–8.
1.
English R, Ruiz S. Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia: Are Biopsy Location, Hair Diameter Diversity, and Relative Hair Follicle Miniaturization Partly to Blame? Clin Cosmet Investig Dermatol. 2021;14:357–65.
Hair loss is a common concern for both men and women. While male-pattern baldness – with its characteristic receding frontal hairline and vertex thinning –…
Call it what you will, androgenetic alopecia, androgenic alopecia, pattern hair loss, or pattern baldness, it has been a part of the human race for…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.