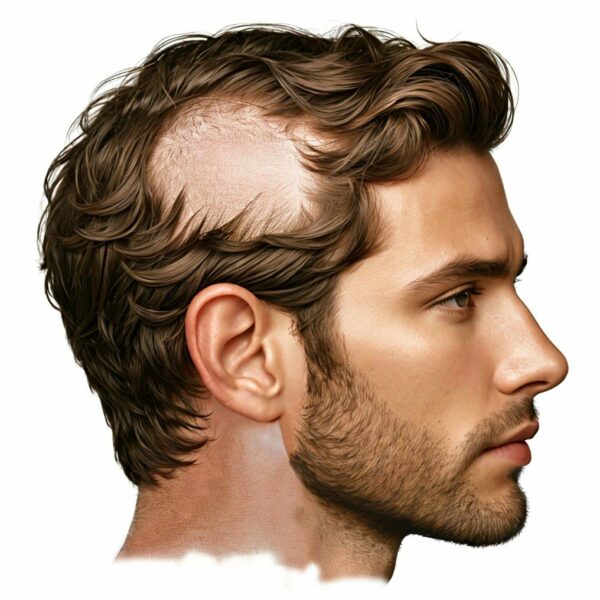
Alopecia areata (AA) is an autoimmune condition characterized by the sudden loss of hair on the scalp and sometimes other parts of the body. It is understood primarily for its effects on hair follicles, leading to hair loss in patches, but its implications on other aspects of skin physiology, such as sweating, are less commonly discussed. This article delves into the intricacies of sweating issues in alopecia areata patients, exploring both the challenges faced and the underlying mechanisms that may contribute to these problems.
Understanding Sweating and Its Importance: Sweating, or perspiration, is a critical physiological process for thermoregulation, allowing the body to maintain its core temperature within a narrow, optimal range. Sweat glands, which are responsible for this function, come in two main types: eccrine and apocrine. Eccrine glands are found throughout the body and play a key role in thermoregulation by secreting sweat directly onto the skin surface, where it evaporates, cooling the body. Apocrine glands, located mainly in areas abundant in hair follicles, such as the armpits and groin, contribute to body odor and are believed to play a role in pheromone release.
Alopecia Areata: It’s useful to quickly review the basics of this autoimmune condition. Alopecia areata manifests as unpredictable hair loss, typically occurring on the scalp but can affect any hair-bearing area of the body. While the exact cause remains elusive, it is widely accepted to involve a complex interplay of genetic, environmental, and immunological factors. The key event is infiltration of inflammatory cells in and around hair follicles. These cells disrupt the ability of the hair follicles to produce hair fiber.
The Connection Between Alopecia Areata and Sweating: Patients with alopecia areata often report abnormalities in sweating, such as reduced sweating (hypohidrosis) or, less commonly, increased sweating (hyperhidrosis). These anomalies can affect their quality of life, exacerbating the psychological distress already associated with hair loss. The exact prevalence of these conditions in AA patients is not well-documented, indicating a gap in our understanding and an area ripe for research.
Mechanisms behind Sweating Issues in AA: The mechanisms linking alopecia areata to altered sweating are complex and multifactorial, involving immune-mediated influences on sweat glands, changes in skin barrier function, and potential nervous system involvement.
Immune-mediated Effects on Sweat Glands: Alopecia areata is an autoimmune disorder wherein cells from the immune system mistakenly attacks hair follicles, leading to hair loss. In alopecia areata, although the autoimmune attack is targeted at hair follicles, the inflammatory cells can indirectly affect the skin’s overall health and its structures, including sweat gland appendages. The mechanisms linking alopecia areata to altered sweating are complex and poorly understood. However, the theory is that the immune cells, while they are busy interfering with hair follicle growth activity, produce a range of chemical signals called cytokines. Cytokines are very small molecules and they easily diffuse through tissues. If they meet with anyt cell that has the relevant receptors to recognize the cytokines, the cells will respond accordingly. Given the close proximity of eccrine glands to hair follicles, especially on the scalp, the cytokines secreted near hair follicles might diffuse through the skin to the nearby sweat glands and inadvertently damage the eccrine gland cells, altering sweat production. Although less is known about autoimmune impacts on apocrine glands, these could also be affected in a similar way due to their association with hair follicles.
Changes in Skin Barrier Function: The absence of hair in alopecia areata can alter skin physiology in several ways that might impact sweating. Hair follicles are not just sites for hair growth; they also play roles in skin barrier function and local immune responses. The loss of hair can change the skin’s microenvironment, potentially affecting the function of nearby sweat glands. Furthermore, hair helps to wick sweat away from the skin, aiding in evaporation and cooling. Without hair, sweat may evaporate less efficiently, potentially leading to perceived changes in sweating.
Nervous System Involvement: The nervous system plays a critical role in regulating sweat production, with sweat gland activity being controlled by sympathetic nerves. Stress and emotional factors, which are often heightened in individuals with alopecia areata due to the psychological impact of the disease, can influence sympathetic nervous system activity. This could lead to anomalies in sweat production, either reducing it due to decreased sympathetic tone in some areas or increasing it in others as a stress response. It should also be noted that inflammation can involve increased production of stress hormones and local alteration of nerve cell secreted factors. It may be possible that these changes in hormones and growth factors can also locally affect sweat gland activity.
Loss of Sweat Glands: It is possible that there is a loss of some sweat glands in people with long term alopecia areata. While hair follicles are able to largely resist permanent destruction, it seems sweat glands might be less robust and there may be some loss in sweat gland density for those who experience alopecia areata over a long time period. However, it’s important to consider that the data to support this possibility is very limited.
Challenges Faced by Patients: The problems with sweating experienced by alopecia areata patients can have several practical and social implications:
Thermoregulatory Issues: Abnormal sweating can impair the body’s ability to regulate temperature, potentially leading to overheating in hot environments or difficulty maintaining warmth in cold conditions. Sometimes this can affect the ability to exercise.
Skin Problems: Compounding the issue, changes in sweating can affect skin hydration and integrity of the scalp skin and may lead to irritation, itching, and even bacterial or fungal infections, further complicating the management of alopecia areata.
Social and Psychological Impact: Given the visible nature of both alopecia areata and sweating issues, individuals may face additional social anxiety and psychological stress, further affecting their quality of life.
Addressing the Issue: Managing sweating issues in alopecia areata involves a multidisciplinary approach:
Topical Treatments: For hyperhidrosis, topical antiperspirants containing aluminum chloride can be effective. In contrast, for hypohidrosis, moisturizers and emollients can help maintain skin hydration.
Systemic Treatments: In some cases, medications that affect the immune system or sympathetic nervous system may be considered to address underlying causes of sweating abnormalities.
Lifestyle Adjustments: Wearing breathable, moisture-wicking fabrics can help manage sweating issues, as can avoiding triggers such as hot environments or spicy foods.
Psychological Support: Counseling or support groups for individuals with alopecia areata can also address the psychological aspects of the condition, potentially mitigating stress-related sweating issues.
Future Research Directions: Research into the specific mechanisms by which alopecia areata affects sweating is ongoing. Greater understanding of these processes may lead to more targeted therapies, improving both hair regrowth prospects and the management of associated symptoms like altered sweating. Collaborative efforts between dermatologists, immunologists, and neurologists are crucial for developing comprehensive care strategies that address the multifaceted challenges faced by patients with alopecia areata.
Conclusion: Sweating poses significant challenges for individuals with alopecia areata, impacting their comfort, confidence, and overall well-being. Understanding the mechanisms underlying sweating in this population is crucial for developing targeted interventions to alleviate these burdens. Further research is needed to elucidate the complex interplay between autoimmune processes, sweat gland function, and psychological factors in alopecia areata, paving the way for more effective management strategies tailored to patients’ needs. By addressing the multifaceted nature of sweating in alopecia areata, healthcare providers can better support individuals navigating the challenges of this autoimmune condition.
Tonkin N, Chavrakov G, Popkhistova E. [Comparative morphometric study of the sebaceous and sweat glands in alopecia areata, chronic diffuse and seborrheic baldness]. Vestn Dermatol Venerol. 1982 Oct;(10):12–5.
1.
Barnhill RL, Goldberg B, Stenn KS. Proliferation of eccrine sweat ducts associated with alopecia areata. J Cutan Pathol. 1988 Feb;15(1):36–9.
1.
Mehregan AH, Mehregan DA. Syringoma-like sweat duct proliferation in scalp alopecias. J Cutan Pathol. 1990 Dec;17(6):355–7.
1.
Elieff D, Sundby S, Kennedy W, Hordinsky M. Decreased sweat-gland number and function in patients with alopecia areata. Br J Dermatol. 1991 Aug;125(2):130–5.
1.
De Berker D, Rees JL. Normal sweat secretion rate in patients with alopecia areata. Br J Dermatol. 1995 Mar;132(3):402–4.
1.
Gilhar A, Paus R, Kalish RS. Lymphocytes, neuropeptides, and genes involved in alopecia areata. J Clin Invest. 2007 Aug;117(8):2019–27.
1.
Poblet E, Jiménez-Acosta F, Hardman JA, Escario E, Paus R. Is the eccrine gland an integral, functionally important component of the human scalp pilosebaceous unit? Exp Dermatol. 2016 Feb;25(2):149–50.
1.
Tan T, Guitart J, Gerami P, Yazdan P. Eccrine Duct Dilation as a Marker of Cicatricial Alopecia. Am J Dermatopathol. 2017 Sept;39(9):668–71.
1.
Poblet E, Jimenez F, Escario-Travesedo E, Hardman JA, Hernández-Hernández I, Agudo-Mena JL, et al. Eccrine sweat glands associate with the human hair follicle within a defined compartment of dermal white adipose tissue. Br J Dermatol. 2018 May;178(5):1163–72.
Alopecia Areata (AA), a condition characterized by hair loss, has been a challenge for humans throughout history. This essay presents a brief tour of the…
Alopecia Areata (AA), a condition marked by hair loss in patches, has been identified and described in numerous ways throughout history, highlighting the evolution of…
Alopecia areata (AA) is a condition characterized by unpredictable hair loss, often occurring in patches. While current science has offered us some insights into the…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.