Syphilis is a chronic, multistage infectious disease caused by the spirochete Treponema pallidum. Known historically as “the great imitator,” syphilis has puzzled clinicians for centuries by mimicking a wide array of dermatological and systemic conditions. Over recent decades, public health authorities and researchers have refocused on syphilis because of its resurgence in various populations and its frequent association with HIV co-infection. Despite advances in treatment and diagnostic testing, syphilis remains a significant global concern, with rising incidence in many parts of the world.
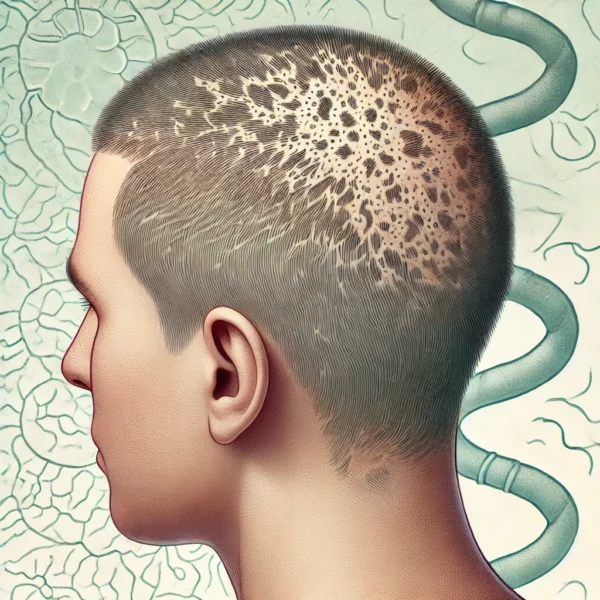
One of the clinical manifestations that can be overlooked or misdiagnosed is hair loss, or “syphilitic alopecia.” While hair loss in syphilis can occur in multiple stages, it is most often recognized during secondary syphilis. Common descriptors such as “moth-eaten” alopecia and “essential syphilitic alopecia” have helped clinicians identify this condition, yet confusion still arises because the pattern of hair loss can resemble other alopecias, including alopecia areata or telogen effluvium. This article provides a detailed overview of syphilis, focusing on epidemiology, pathogen biology, clinical stages, patterns of hair loss, diagnostic methods, differential diagnosis, and contemporary management strategies.
Epidemiology and Recent Trends: Historically, syphilis rates in the general population have waxed and waned in cycles. In the United States, one of the larger spikes occurred during the late 1980s, driven largely by substance use (particularly crack cocaine), followed by a precipitous decline and hitting a minimum in 1999. However, more recently, there has been a resurgence of syphilis in various communities, especially among men who have sex with men (MSM). According to recent surveillance data, cases of primary and secondary syphilis have increased over the past decade in multiple countries, highlighting the need for renewed prevention efforts.
Concurrently, congenital syphilis – syphilis passed from the mother to the fetus during pregnancy – has also been on the rise. Public health experts attribute this resurgence to numerous factors, including reduced access to comprehensive sexual health services, decreased public awareness, and the changing landscape of HIV prevention strategies. The link between syphilis and HIV remains clinically significant, as co-infection can alter the course, severity, and detectability of both infections.
Etiology and Pathogenesis: The causative organism of syphilis, Treponema pallidum, is a thin, spiral-shaped bacterium classified under the order Spirochaetales. It is transmitted primarily through direct contact with infectious lesions (commonly called chancres) or via vertical transmission from mother to fetus. Chancres are typically painless ulcerations that can appear on the genitals, but they may also manifest in extragenital locations such as the lips, mouth, or anus.
Once T. pallidum enters the host, it can spread widely through the bloodstream and lymphatic system. The pathogenesis of syphilis is intimately tied to the microorganism’s ability to evade immune detection; T. pallidum has a relatively sparse outer membrane, allowing it to “hide” from the host immune response. If not treated, the infection can progress from an initial localized lesion to a systemic condition involving skin, bones, cardiovascular structures, and even the central nervous system (CNS).
Clinical Stages of Syphilis: Syphilis progresses through several stages – primary, secondary, latent, and tertiary (also called late) syphilis – each with distinct clinical and pathological features.
Primary Syphilis: The hallmark of primary syphilis is the chancre, a painless ulcer that appears at the site of inoculation (e.g., genitalia, mouth). Regional lymphadenopathy may also be present. The chancre typically resolves spontaneously within three to six weeks, even without treatment.
Secondary Syphilis: If untreated, primary syphilis evolves into secondary syphilis, in which the pathogen spreads systemically through the body. Characteristic findings may include a diffuse rash (commonly involving the palms and soles), mucocutaneous lesions, generalized lymphadenopathy, and systemic symptoms such as fever or malaise. Hair loss, often in a patchy “moth-eaten” distribution, is a recognized but sometimes overlooked feature of secondary syphilis. Rarely, patients may develop an ulcerative form of secondary syphilis known as lues maligna, which is more common in immunocompromised individuals, including those with HIV.
Latent Syphilis: Following secondary syphilis, the disease may enter a latent phase in which there are no overt clinical symptoms. Latent syphilis is subdivided into early (within the first year of infection) and late (beyond one year). During the latent stage, the infection can still progress and eventually enter the tertiary phase.
Tertiary (Late) Syphilis: In untreated individuals, tertiary syphilis can manifest years after the initial infection. Hallmarks of this stage include gummas (soft, non-cancerous growths, sometimes necrotic), cardiovascular involvement (such as aortitis), and neurosyphilis (infection of the central nervous system). When gummas appear on the scalp, localized hair loss may occur overlying these destructive lesions.
Hair Loss in Syphilis: Hair loss, or “syphilitic alopecia,” is most commonly associated with secondary syphilis, although it may also occur in tertiary syphilis when lesions involve hair-bearing areas. Clinicians typically recognize a few classic patterns:
Moth-Eaten Alopecia: The “moth-eaten” pattern is the most well-recognized form of syphilitic hair loss. It is characterized by irregular, patchy areas of hair loss that can mimic alopecia areata, particularly when seen on the scalp. Edges of these patches may appear ragged or indistinct. The process is usually non-scarring, and if syphilis is treated, hair regrowth often occurs.
Essential Syphilitic Alopecia (Diffuse Alopecia): A more subtle pattern, essential syphilitic alopecia occurs when diffuse thinning of the hair is the primary or only manifestation of secondary syphilis, without other obvious cutaneous lesions. Patients may confuse this with telogen effluvium or other forms of diffuse hair thinning, underscoring the need for a thorough physical examination and diagnostic testing.
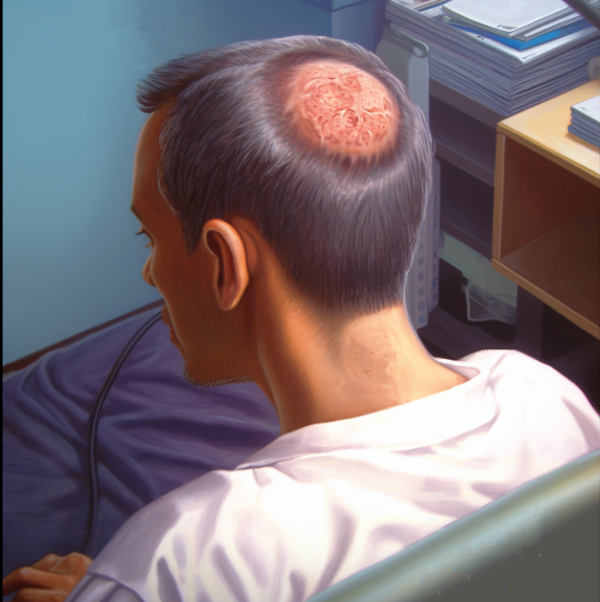
Scalp Involvement in Lues Maligna: Lues maligna, also termed malignant syphilis, is a rare but severe ulceronodular variant of secondary syphilis more frequently associated with immunosuppression (e.g., HIV infection). When the ulcerative lesions involve the scalp, scarring alopecia may result from follicular destruction.
Tertiary Syphilis (Gumma-Related Alopecia): In tertiary disease, gummas can form in various body tissues, including skin. If gummas occur on the scalp, the overlying hair follicles can be destroyed, potentially leading to permanent scarring and hair loss.
Because syphilitic hair loss can imitate other dermatological conditions, early recognition and appropriate serological testing are crucial. A high index of suspicion is particularly important for clinicians when patients present with patchy or diffuse alopecia and other systemic symptoms or risk factors (e.g., multiple sexual partners, concurrent STIs, or HIV infection).
Diagnostic Approach: A combination of clinical evaluation, direct detection techniques, and serological tests is used to confirm a diagnosis of syphilis. In modern practice, two general testing strategies are employed: the traditional screening approach and the “reverse” screening approach.
Traditional Screening Approach: A) Non-Treponemal Tests: The Rapid Plasma Reagin (RPR) and Venereal Disease Research Laboratory (VDRL) tests have historically been the first-line screening tools. They measure antibodies to cardiolipin-cholesterol-lecithin antigens released by damaged cells and T. pallidum. Although sensitive, these tests can yield false-positives due to autoimmune disorders, viral infections, or advanced age. B) Confirmatory Treponemal Tests: If the RPR or VDRL test is reactive, then a confirmatory treponemal test—such as the Fluorescent Treponemal Antibody Absorbed (FTA-ABS) or Treponema pallidum Particle Agglutination (TP-PA) test—is performed to verify the presence of antibodies specific to T. pallidum.
Reverse Screening Approach: Many laboratories now employ a reverse sequence screening algorithm, beginning with automated treponemal enzyme or chemiluminescent immunoassays (EIA/CIA) for T. pallidum IgG or IgM. If this test is reactive, it is followed by a quantitative RPR or VDRL. Discrepancies between the EIA/CIA and RPR may necessitate confirmation with another treponemal test such as TP-PA.
Dark Field Microscopy and Direct Fluorescent Antibody (DFA): In cases of active mucocutaneous lesions, direct visualization of T. pallidum via dark field microscopy or direct fluorescent antibody testing can definitively establish the diagnosis. However, these techniques require experienced personnel and specialized equipment and are therefore less commonly performed.
Biopsy and Histopathology (for Alopecia Lesions): In patients presenting with patchy or diffuse alopecia suspicious for syphilis, a scalp biopsy may show characteristic findings: a primarily perivascular or peribulbar lymphocytic infiltrate, often with plasma cells, and an increased number of hairs in the telogen phase. Special stains, such as the Warthin-Starry stain, may demonstrate spirochetes within tissue.
Differential Diagnosis of Syphilitic Alopecia: The irregular, patchy “moth-eaten” pattern of syphilitic hair loss most closely resembles alopecia areata, which can also present with well-demarcated areas of hair loss. However, alopecia areata patches generally display “exclamation mark” hairs at the periphery and lack additional systemic features suggestive of infection. Essential syphilitic alopecia (diffuse thinning) can also be mistaken for telogen effluvium, androgenetic alopecia, or other causes of diffuse hair shedding. Ultimately, serological testing is critical to distinguish syphilitic alopecia from these mimics.
Treatment and Follow-Up: Treatment of syphilis aims to halt the disease’s progression, reduce transmission, and prevent long-term complications such as neurosyphilis or cardiovascular syphilis. Penicillin G, particularly benzathine penicillin G, is the cornerstone of therapy for all stages of syphilis.
Early Syphilis (Primary, Secondary, Early Latent): The standard response is a single intramuscular injection of benzathine penicillin G, 2.4 million units. This dose effectively clears early infections in most immunocompetent patients.
Late Latent and Tertiary Syphilis (Without Neurosyphilis): Patients may require three weekly injections of benzathine penicillin G, each 2.4 million units (totaling 7.2 million units). This extended regimen is necessary to ensure the eradication of potentially deeper or more extensive tissue involvement.
Neurosyphilis and Ocular Syphilis: Aqueous crystalline penicillin G administered intravenously (18–24 million units per day in divided doses) for 10–14 days is the mainstay of therapy for neurosyphilis. Alternatively, procaine penicillin G plus probenecid may be used in certain scenarios.
HIV Co-Infection: HIV-infected individuals generally receive the same penicillin-based regimens, although some guidelines suggest that more frequent follow-up and additional doses of penicillin might be needed in complicated or advanced cases. Concurrently, optimization of antiretroviral therapy (ART) is essential for patients with HIV.
Penicillin Allergy: For patients with a documented penicillin allergy, alternative regimens include doxycycline (100 mg orally twice daily) or tetracycline (500 mg orally four times daily) for 2–4 weeks, depending on the stage. In pregnancy or neurosyphilis, penicillin desensitization is preferred, since no alternative effectively prevents vertical transmission or treats neurosyphilis as reliably as penicillin.
Jarisch-Herxheimer Reaction: Within the first 24 hours of initiating therapy, patients may experience an acute febrile response known as the Jarisch-Herxheimer reaction, resulting from the rapid killing of T. pallidum. Symptoms include fever, chills, headache, and myalgias. Nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids can help alleviate discomfort.
Monitoring and Follow-Up: Successful treatment is typically gauged by clinical improvement and serial non-treponemal test (RPR, VDRL) titer declines. Patients with early syphilis should be re-evaluated clinically and serologically at 6 and 12 months after treatment. Those with latent or tertiary syphilis should receive follow-up for at least 24 months. A failing decline in titers or recurrence of clinical symptoms may warrant re-treatment or additional investigations for HIV co-infection.
Prognosis and Public Health Considerations: When identified and treated early, syphilis has an excellent prognosis, with resolution of skin lesions, hair regrowth, and prevention of further organ damage. Delayed diagnosis can lead to complications, such as neurosyphilis, cardiovascular involvement, or irreversible damage from gummas. From a public health perspective, contact tracing, partner notification, and routine screening of high-risk groups remain paramount in controlling the spread.
Syphilis is also intricately linked to social determinants of health. Factors such as inadequate access to healthcare, marginalization, and substance use can increase the risk of infection and delay treatment. Comprehensive strategies that address these social barriers—along with regular screening, early intervention, and patient education—are vital for reducing syphilis rates on a wider scale.
Conclusion: Syphilis persists as a dynamic public health challenge due to its complex pathogenesis, often-subtle presentations, and cyclical epidemiological patterns. Hair loss, frequently recognized as the “moth-eaten” alopecia of secondary syphilis, is one of the disease’s more distinctive cutaneous signs but can be misidentified as alopecia areata or sometimes telogen effluvium. Essential syphilitic alopecia and rare ulceronodular forms (lues maligna) further expand the differential diagnosis for hair loss and skin lesions.
Fortunately, T. pallidum remains sensitive to penicillin, rendering proper antibiotic treatment both curative and cost-effective. Rapid detection using modern diagnostic algorithms (reverse and traditional screening approaches) aids in early intervention and helps prevent complications such as neurosyphilis and congenital syphilis. For patients presenting with hair loss and risk factors for syphilis, thorough examination and serologic screening is crucial to avoid diagnostic delay.
van der Willigen AH, Peereboom-Wynia JD, van der Hoek JC, Mulder PG, van Joost TH, Stolz E. Hair root studies in patients suffering from primary and secondary syphilis. Acta Derm Venereol. 1987;67(3):250–4.
1.
Lee JY, Hsu ML. Alopecia syphilitica, a simulator of alopecia areata: histopathology and differential diagnosis. J Cutan Pathol. 1991 Apr;18(2):87–92.
1.
Jordaan HF, Louw M. The moth-eaten alopecia of secondary syphilis. A histopathological study of 12 patients. Am J Dermatopathol. 1995 Apr;17(2):158–62.
Nam-Cha SH, Guhl G, Fernández-Peña P, Fraga J. Alopecia syphilitica with detection of Treponema pallidum in the hair follicle. J Cutan Pathol. 2007 Dec;34 Suppl 1:37–40.
1.
Bi MY, Cohen PR, Robinson FW, Gray JM. Alopecia syphilitica-report of a patient with secondary syphilis presenting as moth-eaten alopecia and a review of its common mimickers. Dermatol Online J. 2009 Oct 15;15(10):6.
1.
Tognetti L, Cinotti E, Perrot JL, Campoli M, Rubegni P. Syphilitic alopecia: uncommon trichoscopic findings. Dermatol Pract Concept. 2017 July 31;7(3):55–9.
1.
García-Montero P, Repiso-Jiménez JB, García-Harana C. Syphilitic Alopecia of the Eyebrows and Eyelashes. Actas Dermosifiliogr (Engl Ed). 2019 Mar;110(2):e12.
1.
Tejapira K, Sakpuwadol N, Pomsoong C, Ratanapokasatit Y, Suchonwanit P. Trichoscopic Features of Syphilitic Alopecia and Alopecia Areata: A Comparative Study. Clin Cosmet Investig Dermatol. 2023;16:2259–69.
Demodex folliculorum is a microscopic mite that inhabits the human pilosebaceous unit and has fascinated, unsettled, and occasionally misled clinicians and patients for more than…
Introduction: Kerion Celsi is a severe, inflammatory form of tinea capitis, primarily affecting children. It is characterized by a boggy, purulent, and sometimes painful lesion…
Introduction: Folliculitis – the inflammation of hair follicles – most commonly arises from bacterial invasion, notably Staphylococcus aureus. However, a spectrum of viral agents can…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.