Hair loss is a common concern for both men and women. While male-pattern baldness – with its characteristic receding frontal hairline and vertex thinning – is widely recognized, many people wonder whether women can experience a similar recession of the hairline. Historically, deep frontoparietal hairline recession in women has been viewed as a sign of pathologic virilization (excess male hormones). However, clinical studies indicate that women may indeed exhibit a receding hairline pattern, particularly as they transition through menopause. This article explores the prevalence, patterns, underlying mechanisms, and clinical implications of hairline recession in women, drawing on foundational research as well as contemporary understanding.
Ludwig Classification of Female Hair Loss: In 1977, Ludwig described three grades of female androgenic alopecia, emphasizing diffuse thinning over the crown while preserving the frontal hairline:
Grade I : Perceptible thinning on the crown, frontal hairline intactGrade II : Pronounced rarefaction within the same central zoneGrade III : Full baldness in that area, frontal margin still preserved Ludwig’s system highlighted that, unlike men, women typically do not lose hair at the frontal hairline. Consequently, any M-shaped frontoparietal recession in a woman was traditionally viewed as abnormal.
Hamilton Classification Adapted to Women: Hamilton’s classification (Types I–VIII) specifically describes male balding patterns, ranging from minimal thinning to advanced vertex and frontal recession. When elements of this pattern – particularly Types II–V, which include deep M-shaped frontoparietal recession – appear in women, they have been labelled “patterned” or “male-pattern” alopecia.
Prevalence of Hairline Recession in Women: Beek first described a rapid-onset, receding–hairline baldness in women in 1946, noting that it typically appeared six to seven months following childbirth or miscarriage. He observed that, unlike diffuse postpartum shedding (what we now recognize as telogen effluvium), this hair loss was transient and generally resolved by nine months. Unfortunately Beek’s commentary was largely ignored and the true significance of his observations did not become apparent until much later.
In a landmark survey of 564 ostensibly healthy white women aged 29–99, Venning and Dawber in 1988 systematically assessed scalp hair distribution in both premenopausal and postmenopausal subjects. Their principal observations were:
Premenopausal women (n = 254): 87 % exhibited Ludwig-type thinning without hairline recession. 13 % showed Hamilton-type frontal or frontoparietal recessionPostmenopausal women (n = 310): 63 % had Ludwig-type patterns. 37 % displayed Hamilton-type recession, including deep M-shaped loss The frequency of “male-pattern” hairline recession in women rose sharply after menopause. Indeed, only about one in eight premenopausal women showed any frontal recession, whereas more than one in three postmenopausal women did. When stratified by decade, the data revealed a clear age effect. The jump in patterned recession coincided with the typical age of menopause (around 50–55 years).
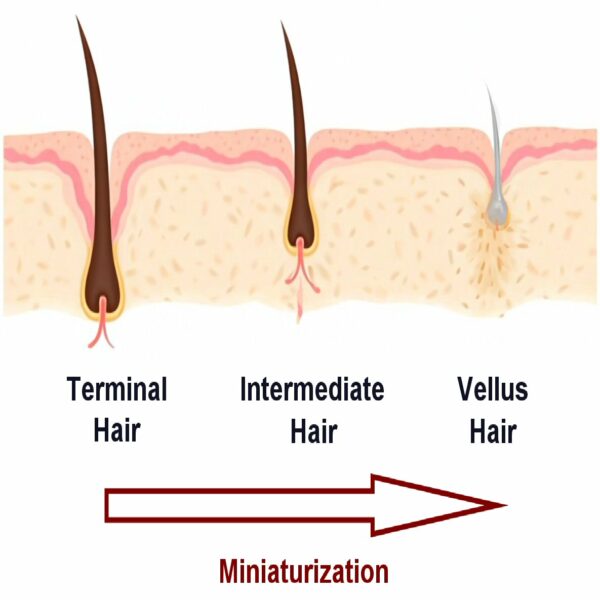
Hormonal Influences: Hair follicle miniaturization – the hallmark of androgenic alopecia – is driven by dihydrotestosterone (DHT) acting on susceptible follicles. In men, circulating androgens rise steadily through adulthood, promoting frontal and vertex thinning. In women, ovarian estrogen production exerts a relative anti-androgenic influence. As estrogen levels decline during the menopausal transition, this protective effect wanes, unmasking the follicular sensitivity to androgens and often precipitating increased hair shedding and patterning.
Virilization vs. Normal Aging: Early dermatologic teaching held that Hamilton-type recession in women signified virilizing disorders (e.g., polycystic ovary syndrome, adrenal hyperplasia, and similar), often accompanied by hirsutism, acne, menstrual irregularities, or elevated serum testosterone. However, Venning and Dawber’s community-based survey found that, in the absence of other virilizing signs, patterned recession is frequently a fairly normal feature more often seen in menopausal women. Thus, hairline recession by itself is not a reliable marker of any endocrine pathology.
Prevalence in Modern Studies: More recent epidemiologic studies – spanning more diverse ethnicities – confirm that frontal thinning and hairline recession are present in a small minority of women, especially beyond menopause. Reported rates of frontal hairline involvement range from 0% in younger cohorts to over 30% in older women. These figures align with the Venning & Dawber observations that hairline recession is more likely to be seen in women from menopause onwards despite differences in study design and population.
Clinical Implications: When a woman presents with frontal hairline recession looking for a diagnosis, clinicians should:
Obtain a thorough history : Age of onset, menopausal status, menstrual regularity, signs of virilization.Perform a clinical examination : Document hair density, recession depth, and associated scalp changes.Assess laboratory parameters if virilizing features are present: Blood serum total and free testosterone, DHEA-S, sex hormone-binding globulin tests can provide important data as to underlying causes of hairline recession in women. Isolated hairline recession in an otherwise healthy, postmenopausal woman often requires no endocrinologic workup.
Management: Several medical therapies are potentially used by dermatologists for treating hairline recession in women:
Topical minoxidil (2 % or 5 % solution): FDA-approved for female pattern hair loss; promotes anagen phase and modest hair regrowth. Oral minoxidil is also now considered for some individuals.Oral anti-androgens (e.g., spironolactone, cyproterone acetate in some countries): Can be considered when hyperandrogenism is documented.Finasteride and dutasteride : Some clinicians consider using these 5-alpha reductase inhibitor drugs for treating androgen related hair loss in post-menopausal women. Hair transplantation : Follicular unit transplantation can restore recession, but donor hair availability and patient expectations must be carefully managed. Differential Diagnosis: When assessing a woman with apparent frontal or frontoparietal thinning, it is essential to distinguish androgenetic patterning from other causes of hair loss. Key entities to consider include:
Alopecia Areata (AA): Presentation: Sudden, well-circumscribed patches of complete hair loss; may progress to more extensive patterns. Examination: “Exclamation-point” hairs at lesion margins; smooth skin without scaling or atrophy; positive hair-pull in active margins. Distinguishing Features: Patchy distribution; preservation of hairline density outside lesions; possibility of nail pitting and other autoimmune clues.Traction Alopecia: Presentation can include frontal and temporal recession in areas subjected to chronic tension (tight braids, ponytails, extensions). Examination often reveals perifollicular erythema or pustules in early stages; broken hairs of varying lengths; eventually leads to permanent scarring if unrelieved. Distinguishing features usually involve a history of hairstyling practices; perifollicular inflammation; improvement upon hairstyle modification. Frontal Fibrosing Alopecia (FFA): Presentation is seen as a progressive, band-like frontal hairline regression, often accompanied by eyebrow loss; predominates in postmenopausal women. Examination shows scarring (smooth, shiny skin), perifollicular erythema, and loss of follicular ostia on trichoscopy. Distinguishing Features with FFA include a scarring pattern; absence of follicular miniaturization; characteristic histologic interface dermatitis. Conclusion: Women can indeed experience a receding hairline reminiscent of male-pattern baldness. While deep frontoparietal recession in women was once thought to be rare and pathognomonic of virilization, population studies demonstrate that up to one-third of postmenopausal women exhibit Hamilton-type hairline recession without other endocrine abnormalities. The menopausal decline in estrogen unbalances the androgen–estrogen interplay, allowing DHT-mediated follicular miniaturization to encroach on the frontal margins. Clinicians should recognize that hairline recession in women often reflects normal aging rather than any hidden disease. A careful history, targeted examination, and selective endocrine evaluation can distinguish benign patterning from true virilizing pathology. A range of medical and cosmetic interventions are available to address both the physical and psychological impacts of hairline recession in women.
Bibliography
11711645 {11711645:FDQ3ANBM},{11711645:JNY8APP9},{11711645:B257YEZ7},{11711645:FGXNIEFN},{11711645:TGU4VD6P},{11711645:S39HUCHJ},{11711645:7EKAHGMX},{11711645:E2T4R365},{11711645:3PXADVR5},{11711645:BFP4DQE5},{11711645:SEVUXWIK},{11711645:SVH99EDT},{11711645:XICXMDFV} 1 vancouver 50 date asc 1829 https://www.keratin.com/wp-content/plugins/zotpress/ %7B%22status%22%3A%22success%22%2C%22updateneeded%22%3Afalse%2C%22instance%22%3Afalse%2C%22meta%22%3A%7B%22request_last%22%3A0%2C%22request_next%22%3A0%2C%22used_cache%22%3Atrue%7D%2C%22data%22%3A%5B%7B%22key%22%3A%22TGU4VD6P%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Birch%20et%20al.%22%2C%22parsedDate%22%3A%222001-02%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BBirch%20MP%2C%20Messenger%20JF%2C%20Messenger%20AG.%20Hair%20density%2C%20hair%20diameter%20and%20the%20prevalence%20of%20female%20pattern%20hair%20loss.%20Br%20J%20Dermatol.%202001%20Feb%3B144%282%29%3A297%26%23x2013%3B304.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Hair%20density%2C%20hair%20diameter%20and%20the%20prevalence%20of%20female%20pattern%20hair%20loss%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%20P.%22%2C%22lastName%22%3A%22Birch%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%20F.%22%2C%22lastName%22%3A%22Messenger%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%20G.%22%2C%22lastName%22%3A%22Messenger%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20Female%20pattern%20hair%20loss%20is%20common%20but%20estimates%20of%20its%20prevalence%20have%20varied%20widely.%20The%20relationships%20between%20the%20clinical%20diagnosis%20of%20female%20pattern%20hair%20loss%20and%20objective%20measurements%20of%20hair%20density%20and%20hair%20diameter%20have%20not%20previously%20been%20evaluated.%5CnOBJECTIVES%3A%20To%20determine%20the%20prevalence%20of%20female%20pattern%20hair%20loss%20and%20to%20relate%20the%20clinical%20findings%20to%20hair%20density%20and%20hair%20diameter.%5CnMETHODS%3A%20We%20examined%20377%20women%2C%20aged%2018--99%20years%2C%20who%20presented%20to%20a%20general%20dermatology%20clinic%20with%20complaints%20unrelated%20to%20hair%20growth%20%28the%20unselected%20sample%29.%20A%20second%20group%20of%2047%20women%20referred%20with%20typical%20female%20pattern%20hair%20loss%20was%20included%20in%20analyses%20of%20the%20relationships%20between%20hair%20density%2C%20hair%20diameter%20and%20the%20clinical%20diagnosis.%20Hair%20density%20was%20measured%20using%20a%20photographic%20method.%20In%20each%20subject%20the%20major%20and%20minor%20axis%20diameters%20were%20measured%20in%20a%20random%20sample%20of%2050%20hairs.%5CnRESULTS%3A%20Six%20per%20cent%20of%20women%20aged%20under%2050%20years%20were%20diagnosed%20as%20having%20female%20pattern%20hair%20loss%2C%20increasing%20to%2038%25%20in%20subjects%20aged%2070%20years%20and%20over.%20The%20mean%20%2B%5C%2F-%20SEM%20hair%20density%20was%20293%20%2B%5C%2F-%2061.3%20hairs%20cm%28-2%29%20at%20age%2035%20years%2C%20falling%20to%20211%20%2B%5C%2F-%2055.1%20hairs%20cm%28-2%29%20at%20age%2070%20years.%20Hair%20density%20showed%20a%20normal%20distribution%20in%20the%20unselected%20sample.%20Most%20women%20classified%20as%20having%20female%20pattern%20hair%20loss%20had%20hair%20densities%20within%20the%20lower%20half%20of%20the%20normal%20distribution.%20The%20perception%20of%20hair%20loss%20was%20determined%20mainly%20by%20low%20hair%20density%20%28ANOVA%20P%20%26lt%3B%200.001%29%2C%20but%20there%20was%20overlap%20in%20hair%20density%20between%20women%20classified%20as%20having%20Ludwig%20I%20hair%20loss%20and%20the%20no%20hair%20loss%20group%2C%20which%20was%20partly%20accounted%20for%20by%20differences%20in%20mean%20hair%20diameter%20%28ANOVA%20P%20%26lt%3B%200.001%29.%20Low%20hair%20density%20was%20associated%20with%20fewer%20hairs%20of%20all%20diameters.%5CnCONCLUSIONS%3A%20Hair%20density%20in%20women%20is%20distributed%20as%20a%20normal%20variable%2C%20indicating%20that%20it%20is%20determined%20as%20a%20multifactorial%20trait.%20Women%20with%20female%20pattern%20hair%20loss%20have%20a%20hair%20density%20which%20falls%20below%20the%20mean%20but%20lies%20within%20the%20spectrum%20of%20the%20normal%20distribution%2C%20although%20other%20factors%2C%20including%20hair%20diameter%2C%20may%20affect%20the%20subjective%20impression%20of%20hair%20loss.%20The%20hair%20diameter%20data%20suggest%20that%20low%20hair%20density%20is%20not%20due%20to%20progressive%20diminution%20in%20hair%20follicle%20size%20and%20that%20follicular%20miniaturization%20may%20occur%20within%20the%20space%20of%20a%20single%20hair%20cycle.%22%2C%22date%22%3A%222001-02%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1046%5C%2Fj.1365-2133.2001.04018.x%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220007-0963%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A58%3A28Z%22%7D%7D%2C%7B%22key%22%3A%22SVH99EDT%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Olsen%22%2C%22parsedDate%22%3A%222001-09%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BOlsen%20EA.%20Female%20pattern%20hair%20loss.%20J%20Am%20Acad%20Dermatol.%202001%20Sept%3B45%283%20Suppl%29%3AS70-80.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Female%20pattern%20hair%20loss%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22E.%20A.%22%2C%22lastName%22%3A%22Olsen%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222001-09%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1067%5C%2Fmjd.2001.117426%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220190-9622%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A29%3A34Z%22%7D%7D%2C%7B%22key%22%3A%227EKAHGMX%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Price%22%2C%22parsedDate%22%3A%222003-06%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BPrice%20VH.%20Androgenetic%20alopecia%20in%20women.%20J%20Investig%20Dermatol%20Symp%20Proc.%202003%20June%3B8%281%29%3A24%26%23x2013%3B7.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Androgenetic%20alopecia%20in%20women%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Vera%20H.%22%2C%22lastName%22%3A%22Price%22%7D%5D%2C%22abstractNote%22%3A%22Androgenetic%20alopecia%20%28AGA%29%2C%20also%20known%20in%20women%20as%20female%20pattern%20hair%20loss%2C%20is%20caused%20by%20androgens%20in%20genetically%20susceptible%20women%20and%20men.%20The%20thinning%20begins%20between%20ages%2012%20and%2040%20years%2C%20the%20inheritance%20pattern%20is%20polygenic%2C%20and%20the%20incidence%20is%20the%20same%20as%20in%20men.%20In%20susceptible%20hair%20follicles%2C%20dihydrotestosterone%20binds%20to%20the%20androgen%20receptor%2C%20and%20the%20hormone-receptor%20complex%20activates%20the%20genes%20responsible%20for%20the%20gradual%20transformation%20of%20large%20terminal%20follicles%20to%20miniaturized%20follicles.%20Both%20young%20women%20and%20young%20men%20with%20AGA%20have%20higher%20levels%20of%205alpha%20reductase%20and%20androgen%20receptor%20in%20frontal%20hair%20follicles%20compared%20to%20occipital%20follicles.%20At%20the%20same%20time%2C%20young%20women%20have%20much%20higher%20levels%20of%20cytochrome%20p-450%20aromatase%20in%20frontal%20follicles%20than%20men%20who%20have%20minimal%20aromatase%2C%20and%20women%20have%20even%20higher%20aromatase%20levels%20in%20occipital%20follicles.%20The%20diagnosis%20of%20AGA%20in%20women%20is%20supported%20by%20early%20age%20of%20onset%2C%20the%20pattern%20of%20increased%20thinning%20over%20the%20frontal%5C%2Fparietal%20scalp%20with%20greater%20density%20over%20the%20occipital%20scalp%2C%20retention%20of%20the%20frontal%20hairline%2C%20and%20the%20presence%20of%20miniaturized%20hairs.%20Most%20women%20with%20AGA%20have%20normal%20menses%20and%20pregnancies.%20Extensive%20hormonal%20testing%20is%20usually%20not%20needed%20unless%20symptoms%20and%20signs%20of%20androgen%20excess%20are%20present%20such%20as%20hirsutism%2C%20severe%20unresponsive%20cystic%20acne%2C%20virilization%2C%20or%20galactorrhea.%20Topical%20minoxidil%20solution%20is%20the%20only%20drug%20available%20for%20promoting%20hair%20growth%20in%20women%20with%20AGA.%20Efficacy%20has%20been%20shown%20in%20double-blind%20studies%20using%20hair%20counts%20and%20hair%20weight.%22%2C%22date%22%3A%222003-06%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1046%5C%2Fj.1523-1747.2003.12168.x%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221087-0024%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A46%3A52Z%22%7D%7D%2C%7B%22key%22%3A%22FGXNIEFN%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Sinclair%22%2C%22parsedDate%22%3A%222004-11%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BSinclair%20R.%20Chronic%20telogen%20effluvium%20or%20early%20androgenetic%20alopecia%3F%20Int%20J%20Dermatol.%202004%20Nov%3B43%2811%29%3A842%26%23x2013%3B3.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Chronic%20telogen%20effluvium%20or%20early%20androgenetic%20alopecia%3F%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rodney%22%2C%22lastName%22%3A%22Sinclair%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222004-11%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1365-4632.2004.02034.x%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220011-9059%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-13T16%3A04%3A53Z%22%7D%7D%2C%7B%22key%22%3A%22E2T4R365%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Rebora%20et%20al.%22%2C%22parsedDate%22%3A%222005-10%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BRebora%20A%2C%20Guarrera%20M%2C%20Baldari%20M%2C%20Vecchio%20F.%20Distinguishing%20androgenetic%20alopecia%20from%20chronic%20telogen%20effluvium%20when%20associated%20in%20the%20same%20patient%3A%20a%20simple%20noninvasive%20method.%20Arch%20Dermatol.%202005%20Oct%3B141%2810%29%3A1243%26%23x2013%3B5.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Distinguishing%20androgenetic%20alopecia%20from%20chronic%20telogen%20effluvium%20when%20associated%20in%20the%20same%20patient%3A%20a%20simple%20noninvasive%20method%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Alfredo%22%2C%22lastName%22%3A%22Rebora%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Marcella%22%2C%22lastName%22%3A%22Guarrera%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Manuela%22%2C%22lastName%22%3A%22Baldari%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Federica%22%2C%22lastName%22%3A%22Vecchio%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20Distinguishing%20chronic%20telogen%20effluvium%20%28CTE%29%20from%20androgenetic%20alopecia%20%28AGA%29%20may%20be%20difficult%20especially%20when%20associated%20in%20the%20same%20patient.%5CnOBSERVATIONS%3A%20One%20hundred%20consecutive%20patients%20with%20hair%20loss%20who%20were%20clinically%20diagnosed%20as%20having%20CTE%2C%20AGA%2C%20AGA%20%2B%20CTE%2C%20or%20remitting%20CTE.%20Patients%20washed%20their%20hair%20in%20the%20sink%20in%20a%20standardized%20way.%20All%20shed%20hairs%20were%20counted%20and%20divided%20%26quot%3Bblindly%26quot%3B%20into%205%20cm%20or%20longer%2C%20intermediate%20length%20%28%26gt%3B3%20to%20%26lt%3B5%20cm%29%2C%20and%203%20cm%20or%20shorter.%20The%20latter%20were%20considered%20telogen%20vellus%20hairs%2C%20and%20patients%20having%20at%20least%2010%25%20of%20them%20were%20classified%20as%20having%20AGA.%20We%20assumed%20that%20patients%20shedding%20200%20hairs%20or%20more%20had%20CTE.%20The%20kappa%20statistic%20revealed%2C%20however%2C%20that%20the%20best%20concordance%20between%20clinical%20and%20numerical%20diagnosis%20%28kappa%20%3D%200.527%29%20was%20obtained%20by%20setting%20the%20cutoff%20shedding%20value%20at%20100%20hairs%20or%20more.%20Of%20the%20100%20patients%2C%2018%20with%2010%25%20or%20more%20of%20hairs%20that%20were%203%20cm%20or%20shorter%20and%20who%20shed%20fewer%20than%20100%20hairs%20were%20diagnosed%20as%20having%20AGA%3B%2034%20with%20fewer%20than%2010%25%20of%20hairs%20that%20were%203%20cm%20or%20shorter%20and%20who%20shed%20at%20least%20100%20hairs%20were%20diagnosed%20as%20having%20CTE%3B%2034%20with%2010%25%20or%20more%20of%20hairs%20that%20were%203%20cm%20or%20shorter%20and%20who%20shed%20at%20least%20100%20hairs%20were%20diagnosed%20as%20having%20AGA%20%2B%20CTE%3B%20and%2014%20with%20fewer%20than%2010%25%20of%20hairs%20that%20were%203%20cm%20or%20shorter%20and%20who%20shed%20fewer%20than%20100%20hairs%20were%20diagnosed%20as%20having%20CTE%20in%20remission.%5CnCONCLUSION%3A%20This%20method%20is%20simple%2C%20noninvasive%2C%20and%20suitable%20for%20office%20evaluation.%22%2C%22date%22%3A%222005-10%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1001%5C%2Farchderm.141.10.1243%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220003-987X%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A44%3A19Z%22%7D%7D%2C%7B%22key%22%3A%22SEVUXWIK%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Camacho-Mart%5Cu00ednez%22%2C%22parsedDate%22%3A%222009-03%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BCamacho-Mart%26%23xED%3Bnez%20FM.%20Hair%20loss%20in%20women.%20Semin%20Cutan%20Med%20Surg.%202009%20Mar%3B28%281%29%3A19%26%23x2013%3B32.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Hair%20loss%20in%20women%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Francisco%20M.%22%2C%22lastName%22%3A%22Camacho-Mart%5Cu00ednez%22%7D%5D%2C%22abstractNote%22%3A%22Female%20pattern%20hair%20loss%20%28FPHL%29%20is%20a%20clinical%20problem%20that%20is%20becoming%20more%20common%20in%20women.%20Female%20alopecia%20with%20androgen%20increase%20is%20called%20female%20androgenetic%20alopecia%20%28FAGA%29%20and%20without%20androgen%20increase%20is%20called%20female%20pattern%20hair%20loss.%20The%20clinical%20picture%20of%20typical%20FAGA%20begins%20with%20a%20specific%20%26quot%3Bdiffuse%20loss%20of%20hair%20from%20the%20parietal%20or%20frontovertical%20areas%20with%20an%20intact%20frontal%20hairline.%26quot%3B%20Ludwig%20called%20this%20process%20%26quot%3Brarefaction.%26quot%3B%20In%20Ludwig%26%23039%3Bs%20classification%20of%20hair%20loss%20in%20women%2C%20progressive%20type%20of%20FAGA%2C%203%20patterns%20were%20described%3A%20grade%20I%20or%20minimal%2C%20grade%20II%20or%20moderate%2C%20and%20grade%20III%20or%20severe.%20Ludwig%20also%20described%20female%20androgenetic%20alopecia%20with%20male%20pattern%20%28FAGA.M%29%20that%20should%20be%20subclassified%20according%20to%20Ebling%26%23039%3Bs%20or%20Hamilton-Norwood%26%23039%3Bs%20classification.%20FAGA.M%20may%20be%20present%20in%204%20conditions%3A%20persistent%20adrenarche%20syndrome%2C%20alopecia%20caused%20by%20an%20adrenal%20or%20an%20ovarian%20tumor%2C%20posthysterectomy%2C%20and%20as%20an%20involutive%20alopecia.%20A%20more%20recent%20classification%20%28Olsen%26%23039%3Bs%20classification%20of%20FPHL%29%20proposes%202%20types%3A%20early-%20and%20late-onset%20with%20or%20without%20excess%20of%20androgens%20in%20each.%20The%20diagnosis%20of%20FPHL%20is%20made%20by%20clinical%20history%2C%20clinical%20examination%2C%20wash%20test%2C%20dermoscopy%2C%20trichoscan%2C%20trichograms%20and%20laboratory%20test%2C%20especially%20androgenic%20determinations.%20Topical%20treatment%20of%20FPHL%20is%20with%20minoxidil%2C%202-5%25%20twice%20daily.%20When%20FPHL%20is%20associated%20with%20high%20levels%20of%20androgens%2C%20systemic%20antiandrogenic%20therapy%20is%20needed.%20Persistent%20adrenarche%20syndrome%20%28adrenal%20SAHA%29%20and%20alopecia%20of%20adrenal%20hyperandrogenism%20is%20treated%20with%20adrenal%20suppression%20and%20antiandrogens.%20Adrenal%20suppression%20is%20achieved%20with%20glucocorticosteroids.%20Antiandrogens%20therapy%20includes%20cyproterone%20acetate%2C%20drospirenone%2C%20spironolactone%2C%20flutamide%2C%20and%20finasteride.%20Excess%20release%20of%20ovarian%20androgens%20%28ovarian%20SAHA%29%20and%20alopecia%20of%20ovarian%20hyperandrogenism%20is%20treated%20with%20ovarian%20suppression%20and%20antiandrogens.%20Ovarian%20suppression%20includes%20the%20use%20of%20contraceptives%20containing%20an%20estrogen%2C%20ethinylestradiol%2C%20and%20a%20progestogen.%20Antiandrogens%20such%20as%20cyproterone%20acetate%2C%20always%20accompanied%20by%20tricyclic%20contraceptives%2C%20are%20the%20best%20choice%20of%20antiandrogens%20to%20use%20in%20patients%20with%20FPHL.%20Gonadotropin-releasing%20hormone%20agonists%20such%20as%20leuprolide%20acetate%20suppress%20pituitary%20and%20gonadal%20function%20through%20a%20reduction%20in%20luteinizing%20hormone%20and%20follicle-stimulating%20hormone%20levels.%20Subsequently%2C%20ovarian%20steroid%20levels%20also%20will%20be%20reduced%2C%20especially%20in%20patients%20with%20polycystic%20ovary%20syndrome.%20When%20polycystic%20ovary%20syndrome%20is%20associated%20with%20insulin%20resistance%2C%20metformin%20must%20be%20considered%20as%20treatment.%20Hyperprolactinemic%20SAHA%20and%20alopecia%20of%20pituitary%20hyperandrogenism%20should%20be%20treated%20with%20bromocriptine%20or%20cabergoline.%20Postmenopausal%20alopecia%2C%20with%20previous%20high%20levels%20of%20androgens%20or%20with%20prostatic-specific%20antigen%20greater%20than%200.04%20ng%5C%2FmL%2C%20improves%20with%20finasteride%20or%20dutasteride.%20Although%20we%20do%20not%20know%20the%20reason%2C%20postmenopausal%20alopecia%20in%20normoandrogenic%20women%20also%20improves%20with%20finasteride%20or%20dutasteride%20at%20a%20dose%20of%202.5%20mg%20per%20day.%20Dermatocosmetic%20concealment%20with%20a%20hairpiece%2C%20hair%20prosthesis%20as%20extensions%2C%20or%20partial%20hairpieces%20can%20be%20useful.%20Lastly%2C%20weight%20loss%20undoubtedly%20improves%20hair%20loss%20in%20hyperandrogenic%20women.%22%2C%22date%22%3A%222009-03%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.sder.2009.01.001%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221558-0768%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A29%3A47Z%22%7D%7D%2C%7B%22key%22%3A%22FDQ3ANBM%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Su%20et%20al.%22%2C%22parsedDate%22%3A%222013-08%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BSu%20LH%2C%20Chen%20LS%2C%20Chen%20HH.%20Factors%20associated%20with%20female%20pattern%20hair%20loss%20and%20its%20prevalence%20in%20Taiwanese%20women%3A%20a%20community-based%20survey.%20J%20Am%20Acad%20Dermatol.%202013%20Aug%3B69%282%29%3Ae69-77.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Factors%20associated%20with%20female%20pattern%20hair%20loss%20and%20its%20prevalence%20in%20Taiwanese%20women%3A%20a%20community-based%20survey%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Lin-Hui%22%2C%22lastName%22%3A%22Su%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Li-Sheng%22%2C%22lastName%22%3A%22Chen%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Hsiu-Hsi%22%2C%22lastName%22%3A%22Chen%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20Although%20female%20pattern%20hair%20loss%20%28FPHL%29%20has%20been%20considered%20simply%20the%20female%20counterpart%20of%20male%20pattern%20hair%20loss%20in%20men%2C%20the%20risk%20factors%20may%20differ.%5CnOBJECTIVE%3A%20We%20sought%20to%20evaluate%20factors%20associated%20with%20FPHL%20and%20to%20estimate%20its%20prevalence%20in%20women.%5CnMETHOD%3A%20In%20total%2C%2026%2C226%20subjects%20aged%2030%20years%20and%20older%20participated%20in%20a%20cross-sectional%20survey.%20Ludwig%20and%20Norwood%20classifications%20were%20used%20to%20assess%20the%20degree%20of%20hair%20loss.%20Information%20on%20possible%20risk%20factors%20for%20FPHL%20was%20collected%20using%20a%20questionnaire%20interview.%5CnRESULTS%3A%20The%20prevalence%20of%20FPHL%20%28Ludwig%20grade%20%26gt%3BI%29%20for%20all%20ages%20was%2011.8%25%20%2895%25%20CI%2011.5%25-12.2%25%29%2C%20increasing%20with%20advancing%20age.%20After%20controlling%20for%20age%20and%20family%20history%2C%20statistically%20significant%20associations%20were%20noted%20between%20FPHL%20and%20high%20fasting%20glucose%20%28odds%20ratio%20%5BOR%5D%201.15%2C%2095%25%20confidence%20interval%20%5BCI%5D%201.04-1.28%29%2C%20fewer%20childbirths%20%28OR%201.24%2C%2095%25%20CI%201.12-1.38%29%2C%20breast-feeding%20%28OR%200.88%2C%2095%25%20CI%200.78-0.98%29%2C%20oral%20contraceptive%20use%20%28OR%201.21%2C%2095%25%20CI%201.01-1.45%29%2C%20and%20ultraviolet%20exposure%20more%20than%2016%20hours%20per%20week%20%28OR%201.12%2C%2095%25%20CI%201.02-1.22%29.%5CnLIMITATIONS%3A%20The%20validity%20and%20reliability%20of%20FPHL%20classification%20may%20be%20not%20perfect%20in%20this%20survey%20and%20may%20need%20to%20be%20verified.%20Information%20on%20family%20history%20may%20be%20still%20subject%20to%20recall%20bias.%5CnCONCLUSIONS%3A%20Risk%20factors%20for%20FPHL%20and%20male%20androgenic%20alopecia%20may%20differ.%22%2C%22date%22%3A%222013-08%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.jaad.2012.09.046%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221097-6787%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222025-05-08T16%3A03%3A13Z%22%7D%7D%2C%7B%22key%22%3A%22JNY8APP9%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Herskovitz%20and%20Tosti%22%2C%22parsedDate%22%3A%222013-10%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BHerskovitz%20I%2C%20Tosti%20A.%20Female%20pattern%20hair%20loss.%20Int%20J%20Endocrinol%20Metab.%202013%20Oct%3B11%284%29%3Ae9860.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Female%20pattern%20hair%20loss%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ingrid%22%2C%22lastName%22%3A%22Herskovitz%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Antonella%22%2C%22lastName%22%3A%22Tosti%22%7D%5D%2C%22abstractNote%22%3A%22CONTEXT%3A%20Female%20pattern%20hair%20loss%20%28FPHL%29%20also%20known%20as%20female%20androgenetic%20alopecia%20is%20a%20common%20condition%20afflicting%20millions%20of%20women%20that%20can%20be%20cosmetically%20disrupting.%20Prompt%20diagnosis%20and%20treatment%20are%20essential%20for%20obtaining%20optimal%20outcome.%20This%20review%20addresses%20the%20clinical%20presentation%20of%20female%20pattern%20hair%20loss%2C%20its%20differential%20diagnosis%20and%20treatment%20modalities.%5CnEVIDENCE%20ACQUISITION%3A%20A%29%20Diffuse%20thinning%20of%20the%20crown%20region%20with%20preservation%20of%20the%20frontal%20hairline%20%28Ludwig%26%23039%3Bs%20type%29%20B%29%20The%20%26quot%3BChristmas%20tree%20pattern%26quot%3B%20where%20the%20thinning%20is%20wider%20in%20the%20frontal%20scalp%20giving%20the%20alopecic%20area%20a%20triangular%20shaped%20figure%20resembling%20a%20christmas%20tree.%20C%29%20Thinning%20associated%20with%20bitemporal%20recession%20%28Hamilton%20type%29.%20Generally%2C%20FPHL%20is%20not%20associated%20with%20elevated%20androgens.%20Less%20commonly%20females%20with%20FPHL%20may%20have%20other%20skin%20or%20general%20signs%20of%20hyperandrogenism%20such%20as%20hirsutism%2C%20acne%2C%20irregular%20menses%2C%20infertility%2C%20galactorrhea%20and%20insulin%20resistance.%20The%20most%20common%20endocrinological%20abnormality%20associated%20with%20FPHL%20is%20polycystic%20ovarian%20syndrome%20%28PCOS%29.%5CnRESULTS%3A%20The%20most%20important%20diseases%20to%20consider%20in%20the%20differential%20diagnosis%20of%20FPHL%20include%20Chronic%20Telogen%20Effluvium%20%28CTE%29%2C%20Permanent%20Alopecia%20after%20Chemotherapy%20%28PAC%29%2C%20Alopecia%20Areata%20Incognito%20%28AAI%29%20and%20Frontal%20Fibrosing%20Alopecia%20%28FFA%29.%20This%20review%20describes%20criteria%20for%20distinguishing%20these%20conditions%20from%20FPHL.%5CnCONCLUSIONS%3A%20The%20only%20approved%20treatment%20for%20FPHL%2C%20which%20is%202%25%20topical%20Minoxidil%2C%20should%20be%20applied%20at%20the%20dosage%20of%201ml%20twice%20day%20for%20a%20minimum%20period%20of%2012%20months.%20This%20review%20will%20discuss%20off-label%20alternative%20modalities%20of%20treatment%20including%205-alfa%20reductase%20inhibitors%2C%20antiandrogens%2C%20estrogens%2C%20prostaglandin%20analogs%2C%20lasers%2C%20light%20treatments%20and%20hair%20transplantation.%22%2C%22date%22%3A%222013-10%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.5812%5C%2Fijem.9860%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221726-913X%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222025-05-08T15%3A54%3A38Z%22%7D%7D%2C%7B%22key%22%3A%22S39HUCHJ%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Perez-Mora%20et%20al.%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BPerez-Mora%20N%2C%20Goren%20A%2C%20Velasco%20C%2C%20Bermudez%20F.%20Acute%20telogen%20effluvium%20onset%20event%20is%20associated%20with%20the%20presence%20of%20female%20androgenetic%20alopecia%3A%20potential%20therapeutic%20implications.%20Dermatol%20Ther.%202014%3B27%283%29%3A159%26%23x2013%3B62.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Acute%20telogen%20effluvium%20onset%20event%20is%20associated%20with%20the%20presence%20of%20female%20androgenetic%20alopecia%3A%20potential%20therapeutic%20implications%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Nicolas%22%2C%22lastName%22%3A%22Perez-Mora%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andy%22%2C%22lastName%22%3A%22Goren%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Carlos%22%2C%22lastName%22%3A%22Velasco%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Fernando%22%2C%22lastName%22%3A%22Bermudez%22%7D%5D%2C%22abstractNote%22%3A%22Acute%20telogen%20effluvium%20%28ATE%29%20is%20often%20associated%20with%20female%20androgenetic%20alopecia%20%28FAA%29%2C%20but%20predictive%20factors%20of%20ATE-FAA%20association%20and%20clinical%20factors%20or%20therapies%20that%20may%20influence%20the%20progression%20of%20ATE%20to%20chronic%20telogen%20effluvium%20%28CTE%29%20have%20not%20been%20reported.%20We%20have%20identified%20predictive%20factors%20of%20ATE-FAA%20association%20and%20retrospectively%20evaluated%20the%20impact%20of%20therapies%20on%20the%20progression%20to%20CTE.%20Conclusions%20are%20as%20follows%3A%20%28i%29%20Triggering%20cause%20is%20a%20significant%20independent%20factor%20that%20predicts%20association%20of%20ATE%20with%20FAA.%20%28ii%29%20Triggering%20causes%20with%20higher%20risk%20of%20concurrent%20FAA%20are%20severe%20diet%2C%20iron%20deficiency%2C%20and%20thyroid%20dysfunction.%20%28iii%29%20Patients%20suffering%20ATE%20may%20benefit%20from%20different%20therapeutic%20approaches%20%28depending%20on%20which%20is%20the%20triggering%20cause%29%20to%20prevent%20or%20treat%20the%20association%20with%20FAA.%20%28iv%29%20Minoxidil%20use%20shows%20a%20trend%20to%20lower%20the%20percentage%20of%20progression%20to%20CTE.%20%28v%29%20Apart%20from%20treating%20the%20precipitating%20cause%2C%20the%20different%20additional%20oral%20treatments%20used%20have%20not%20shown%20any%20correlation%20with%20progression%20to%20CTE.%22%2C%22date%22%3A%222014%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1111%5C%2Fdth.12101%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221529-8019%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A53%3A39Z%22%7D%7D%2C%7B%22key%22%3A%223PXADVR5%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Ramos%20and%20Miot%22%2C%22parsedDate%22%3A%222015%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BRamos%20PM%2C%20Miot%20HA.%20Female%20Pattern%20Hair%20Loss%3A%20a%20clinical%20and%20pathophysiological%20review.%20An%20Bras%20Dermatol.%202015%3B90%284%29%3A529%26%23x2013%3B43.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Female%20Pattern%20Hair%20Loss%3A%20a%20clinical%20and%20pathophysiological%20review%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Paulo%20M%5Cu00fcller%22%2C%22lastName%22%3A%22Ramos%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22H%5Cu00e9lio%20Amante%22%2C%22lastName%22%3A%22Miot%22%7D%5D%2C%22abstractNote%22%3A%22Female%20Pattern%20Hair%20Loss%20or%20female%20androgenetic%20alopecia%20is%20the%20main%20cause%20of%20hair%20loss%20in%20adult%20women%20and%20has%20a%20major%20impact%20on%20patients%26%23039%3B%20quality%20of%20life.%20It%20evolves%20from%20the%20progressive%20miniaturization%20of%20follicles%20that%20lead%20to%20a%20subsequent%20decrease%20of%20the%20hair%20density%2C%20leading%20to%20a%20non-scarring%20diffuse%20alopecia%2C%20with%20characteristic%20clinical%2C%20dermoscopic%20and%20histological%20patterns.%20In%20spite%20of%20the%20high%20frequency%20of%20the%20disease%20and%20the%20relevance%20of%20its%20psychological%20impact%2C%20its%20pathogenesis%20is%20not%20yet%20fully%20understood%2C%20being%20influenced%20by%20genetic%2C%20hormonal%20and%20environmental%20factors.%20In%20addition%2C%20response%20to%20treatment%20is%20variable.%20In%20this%20article%2C%20authors%20discuss%20the%20main%20clinical%2C%20epidemiological%20and%20pathophysiological%20aspects%20of%20female%20pattern%20hair%20loss.%22%2C%22date%22%3A%222015%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1590%5C%2Fabd1806-4841.20153370%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221806-4841%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A36%3A55Z%22%7D%7D%2C%7B%22key%22%3A%22XICXMDFV%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Treister-Goltzman%20et%20al.%22%2C%22parsedDate%22%3A%222022-03%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BTreister-Goltzman%20Y%2C%20Yarza%20S%2C%20Peleg%20R.%20Iron%20Deficiency%20and%20Nonscarring%20Alopecia%20in%20Women%3A%20Systematic%20Review%20and%20Meta-Analysis.%20Skin%20Appendage%20Disord.%202022%20Mar%3B8%282%29%3A83%26%23x2013%3B92.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Iron%20Deficiency%20and%20Nonscarring%20Alopecia%20in%20Women%3A%20Systematic%20Review%20and%20Meta-Analysis%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Yulia%22%2C%22lastName%22%3A%22Treister-Goltzman%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Shaked%22%2C%22lastName%22%3A%22Yarza%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Roni%22%2C%22lastName%22%3A%22Peleg%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20There%20is%20no%20clear-cut%20evidence%20in%20the%20existing%20medical%20literature%20of%20an%20association%20between%20iron%20deficiency%20and%20nonscarring%20alopecia.%5CnOBJECTIVE%3A%20The%20objective%20of%20the%20study%20was%20to%20conduct%20a%20systematic%20review%20of%20the%20medical%20literature%20on%20the%20prevalence%20of%20iron%20deficiency%20in%20women%20with%20nonscarring%20alopecia%20and%20compare%20their%20ferritin%20levels%20with%20those%20of%20women%20without%20this%20condition.%5CnMETHODS%3A%20The%20electronic%20databases%20PubMed%2C%20Scopus%2C%20and%20Web%20of%20Science%20were%20searched%20between%20June%2015%2C%202019%2C%20and%20July%2024%2C%202019.%20Studies%20that%20evaluated%20the%20prevalence%20of%20iron%20deficiency%20in%20women%20with%20nonscarring%20alopecia%20and%5C%2For%20compared%20ferritin%20levels%20in%20women%20with%20and%20without%20this%20condition%20were%20entered%20into%20the%20meta-analysis.%20Thirty-six%20of%20928%20identified%20studies%20entered%20the%20systematic%20meta-analysis.%20The%20meta-analysis%20was%20performed%20using%20the%20random-effects%20method.%5CnRESULTS%3A%20The%20overall%20number%20of%20participants%20was%2010%2C029.%20The%20prevalence%20of%20ferritin%20levels%20from%2010%20to%2015%20ng%5C%2FdL%20and%20below%20was%2021%25%20%2812%3B%2029%29.%20Women%20with%20nonscarring%20alopecia%20had%20lower%20ferritin%20values%20at%20MD%20%3D%20-18.51%20ng%5C%2FdL%20%28-25.85%3B%20-11.16%2C%20p%20%26lt%3B%200.01%29.%5CnCONCLUSION%3A%20Women%20with%20hair%20loss%20can%20benefit%20from%20higher%20ferritin%20levels.%22%2C%22date%22%3A%222022-03%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1159%5C%2F000519952%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%222296-9195%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A28%3A37Z%22%7D%7D%2C%7B%22key%22%3A%22BFP4DQE5%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Cussen%20et%20al.%22%2C%22parsedDate%22%3A%222022-08%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BCussen%20L%2C%20McDonnell%20T%2C%20Bennett%20G%2C%20Thompson%20CJ%2C%20Sherlock%20M%2C%20O%26%23x2019%3BReilly%20MW.%20Approach%20to%20androgen%20excess%20in%20women%3A%20Clinical%20and%20biochemical%20insights.%20Clin%20Endocrinol%20%28Oxf%29.%202022%20Aug%3B97%282%29%3A174%26%23x2013%3B86.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Approach%20to%20androgen%20excess%20in%20women%3A%20Clinical%20and%20biochemical%20insights%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Leanne%22%2C%22lastName%22%3A%22Cussen%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Tara%22%2C%22lastName%22%3A%22McDonnell%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Gillian%22%2C%22lastName%22%3A%22Bennett%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Christopher%20J.%22%2C%22lastName%22%3A%22Thompson%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mark%22%2C%22lastName%22%3A%22Sherlock%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Michael%20W.%22%2C%22lastName%22%3A%22O%27Reilly%22%7D%5D%2C%22abstractNote%22%3A%22Androgen%20excess%20in%20women%20typically%20presents%20clinically%20with%20hirsutism%2C%20acne%20or%20androgenic%20alopecia.%20In%20the%20vast%20majority%20of%20cases%2C%20the%20underlying%20aetiology%20is%20polycystic%20ovary%20syndrome%20%28PCOS%29%2C%20a%20common%20chronic%20condition%20that%20affects%20up%20to%2010%25%20of%20all%20women.%20Identification%20of%20women%20with%20non-PCOS%20pathology%20within%20large%20cohorts%20of%20patients%20presenting%20with%20androgen%20excess%20represents%20a%20diagnostic%20challenge%20for%20the%20endocrinologist%2C%20and%20rare%20pathology%20including%20nonclassic%20congenital%20adrenal%20hyperplasia%2C%20severe%20insulin%20resistance%20syndromes%2C%20Cushing%26%23039%3Bs%20disease%20or%20androgen-secreting%20tumours%20of%20the%20ovary%20or%20adrenal%20gland%20may%20be%20missed%20in%20the%20absence%20of%20a%20pragmatic%20screening%20approach.%20Detailed%20clinical%20history%2C%20physical%20examination%20and%20biochemical%20phenotyping%20are%20critical%20in%20risk-stratifying%20women%20who%20are%20at%20the%20highest%20risk%20of%20non-PCOS%20disorders.%20Red%20flag%20features%20such%20as%20rapid%20onset%20symptoms%2C%20overt%20virilization%2C%20postmenopausal%20onset%20or%20severe%20biochemical%20disturbances%20should%20prompt%20investigations%20for%20underlying%20neoplastic%20pathology%2C%20including%20dynamic%20testing%20and%20imaging%20where%20appropriate.%20This%20review%20will%20outline%20a%20proposed%20diagnostic%20approach%20to%20androgen%20excess%20in%20women%2C%20including%20an%20introduction%20to%20androgen%20metabolism%20and%20provision%20of%20a%20suggested%20algorithmic%20strategy%20to%20identify%20non-PCOS%20pathology%20according%20to%20clinical%20and%20biochemical%20phenotype.%22%2C%22date%22%3A%222022-08%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1111%5C%2Fcen.14710%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221365-2265%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222024-08-09T16%3A30%3A46Z%22%7D%7D%2C%7B%22key%22%3A%22B257YEZ7%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Sakpuwadol%20et%20al.%22%2C%22parsedDate%22%3A%222023%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BSakpuwadol%20N%2C%20Tejapira%20K%2C%20Kositkuljorn%20C%2C%20Pomsoong%20C%2C%20Suchonwanit%20P.%20Differences%20in%20Demographic%20and%20Clinical%20Characteristics%20Among%20Subtypes%20of%20Female%20Pattern%20Hair%20Loss.%20Clin%20Cosmet%20Investig%20Dermatol.%202023%3B16%3A2073%26%23x2013%3B82.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Differences%20in%20Demographic%20and%20Clinical%20Characteristics%20Among%20Subtypes%20of%20Female%20Pattern%20Hair%20Loss%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Nawara%22%2C%22lastName%22%3A%22Sakpuwadol%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Kasama%22%2C%22lastName%22%3A%22Tejapira%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Chaninan%22%2C%22lastName%22%3A%22Kositkuljorn%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Cherrin%22%2C%22lastName%22%3A%22Pomsoong%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Poonkiat%22%2C%22lastName%22%3A%22Suchonwanit%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20Female%20pattern%20hair%20loss%20%28FPHL%29%20is%20the%20most%20common%20hair%20loss%20disorder%20in%20women%20that%20can%20be%20classified%20into%20three%20patterns%2C%20including%20Ludwig%2C%20Olsen%2C%20and%20Hamilton-Norwood%20subtypes.%20Information%20regarding%20the%20comparison%20of%20demographics%2C%20clinical%20characteristics%2C%20and%20associated%20comorbidities%20among%20subtypes%20of%20FPHL%20is%20scarce%20and%20contradictory.%5CnOBJECTIVE%3A%20To%20evaluate%20and%20compare%20the%20epidemiology%2C%20clinical%20manifestations%2C%20and%20comorbid%20conditions%20of%20FPHL%20subtypes%20and%20determine%20their%20associated%20factors.%5CnMETHODS%3A%20This%20retrospective%20study%20included%20patients%20who%20were%20diagnosed%20with%20FPHL%20between%20January%202000%20and%20November%202021.%20Participants%20were%20classified%20into%20three%20subtypes%2C%20namely%20Ludwig%2C%20Olsen%2C%20and%20Hamilton-Norwood%2C%20and%20were%20statistically%20compared.%20Variables%20significantly%20associated%20with%20each%20FPHL%20subtype%20were%20identified%20using%20multivariable%20multinomial%20logistic%20regression%20analysis.%5CnRESULTS%3A%20Among%20the%20519%20patients%20with%20FPHL%2C%20the%20Ludwig%20subtype%20was%20the%20most%20prevalent%20%2851.1%25%29%2C%20followed%20by%20the%20Olsen%20%2832.9%25%29%20and%20Hamilton-Norwood%20%2816%25%29%20subtypes.%20The%20Hamilton-Norwood%20subtype%20revealed%20significantly%20higher%20frequencies%20of%20early%20disease%20onset%20%2861.4%25%29%2C%20menstrual%20irregularity%20%2822.9%25%29%2C%20polycystic%20ovary%20syndrome%20%28PCOS%2C%2018.1%25%29%2C%20and%20seborrhea%20%2830.1%25%29%20but%20lower%20frequencies%20of%20overweight%20%2824.1%25%29%20and%20type%202%20diabetes%20mellitus%20%28DM%2C%202.4%25%29.%20Multivariable%20multinomial%20regression%20analysis%20demonstrated%20that%20the%20Hamilton-Norwood%20subtype%20was%20a%20predictor%20for%20early%20disease%20onset%20and%20PCOS%20compared%20to%20Ludwig%20%28early%20onset%3A%20odds%20ratio%20%28OR%29%20%3D%202.14%2C%2095%25%20confidence%20interval%20%28CI%29%20%3D%201.39-4.22%2C%20P%20%3D%200.02%3B%20PCOS%3A%20OR%20%3D%202.02%2C%2095%25%20CI%20%3D%201.55-4.84%2C%20P%20%3D%200.03%29%2C%20and%20Olsen%20%28early%20onset%3A%20OR%20%3D%201.89%2C%2095%25%20CI%20%3D%201.03-3.92%2C%20P%20%3D%200.04%3B%20PCOS%3A%20OR%20%3D%202.24%2C%2095%25%20CI%20%3D%201.89-5.31%2C%20P%20%3D%200.01%29.%20In%20contrast%2C%20the%20Hamilton-Norwood%20pattern%20was%20at%20decreased%20risk%20for%20type%202%20DM%20compared%20to%20Ludwig%20%28OR%20%3D%200.51%2C%2095%25%20CI%20%3D%200.03-0.82%2C%20P%20%3D%200.02%29%2C%20and%20Olsen%20%28OR%20%3D%200.68%2C%2095%25%20CI%20%3D%200.04-0.79%2C%20P%20%3D%200.03%29.%5CnCONCLUSION%3A%20The%20Ludwig%20pattern%20was%20found%20to%20be%20the%20most%20prevalent%20FPHL%20subtype%20among%20Thai%20patients.%20Moreover%2C%20the%20Hamilton-Norwood%20subtype%20was%20associated%20with%20early%20disease%20onset%20and%20PCOS%2C%20whereas%20the%20Ludwig%20and%20Olsen%20subtypes%20were%20associated%20with%20type%202%20DM.%22%2C%22date%22%3A%222023%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.2147%5C%2FCCID.S422335%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221178-7015%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22ZBJKD45I%22%5D%2C%22dateModified%22%3A%222025-05-08T15%3A41%3A49Z%22%7D%7D%5D%7D 1.
Birch MP, Messenger JF, Messenger AG. Hair density, hair diameter and the prevalence of female pattern hair loss. Br J Dermatol. 2001 Feb;144(2):297–304.
1.
Olsen EA. Female pattern hair loss. J Am Acad Dermatol. 2001 Sept;45(3 Suppl):S70-80.
1.
Price VH. Androgenetic alopecia in women. J Investig Dermatol Symp Proc. 2003 June;8(1):24–7.
1.
Sinclair R. Chronic telogen effluvium or early androgenetic alopecia? Int J Dermatol. 2004 Nov;43(11):842–3.
1.
Rebora A, Guarrera M, Baldari M, Vecchio F. Distinguishing androgenetic alopecia from chronic telogen effluvium when associated in the same patient: a simple noninvasive method. Arch Dermatol. 2005 Oct;141(10):1243–5.
1.
Camacho-Martínez FM. Hair loss in women. Semin Cutan Med Surg. 2009 Mar;28(1):19–32.
1.
Su LH, Chen LS, Chen HH. Factors associated with female pattern hair loss and its prevalence in Taiwanese women: a community-based survey. J Am Acad Dermatol. 2013 Aug;69(2):e69-77.
1.
Herskovitz I, Tosti A. Female pattern hair loss. Int J Endocrinol Metab. 2013 Oct;11(4):e9860.
1.
Perez-Mora N, Goren A, Velasco C, Bermudez F. Acute telogen effluvium onset event is associated with the presence of female androgenetic alopecia: potential therapeutic implications. Dermatol Ther. 2014;27(3):159–62.
1.
Ramos PM, Miot HA. Female Pattern Hair Loss: a clinical and pathophysiological review. An Bras Dermatol. 2015;90(4):529–43.
1.
Treister-Goltzman Y, Yarza S, Peleg R. Iron Deficiency and Nonscarring Alopecia in Women: Systematic Review and Meta-Analysis. Skin Appendage Disord. 2022 Mar;8(2):83–92.
1.
Cussen L, McDonnell T, Bennett G, Thompson CJ, Sherlock M, O’Reilly MW. Approach to androgen excess in women: Clinical and biochemical insights. Clin Endocrinol (Oxf). 2022 Aug;97(2):174–86.
1.
Sakpuwadol N, Tejapira K, Kositkuljorn C, Pomsoong C, Suchonwanit P. Differences in Demographic and Clinical Characteristics Among Subtypes of Female Pattern Hair Loss. Clin Cosmet Investig Dermatol. 2023;16:2073–82.