Introduction: Hirsutism, characterized by excessive terminal hair growth in women in a male-pattern distribution, is a common clinical condition with significant psychological and social implications. The Ferriman-Gallwey score (FG score) is the most widely used method for the clinical evaluation of hirsutism. This scoring system, originally developed in 1961 by David Ferriman and John Gallwey, provides a standardized approach to quantify hair growth in women, facilitating diagnosis, treatment decisions, and monitoring of therapeutic efficacy. This article explores the development, methodology, clinical relevance, and limitations of the Ferriman-Gallwey score, offering a comprehensive understanding of its role in managing hirsutism.
Development of the Ferriman-Gallwey Score: The Ferriman-Gallwey score emerged from the need for a systematic and objective method to assess hirsutism. Before its development, clinicians lacked a standardized approach, leading to inconsistencies in diagnosis and treatment. Ferriman and Gallwey aimed to create a reproducible scoring system that could be easily and quickly applied in clinical settings. They evaluated hair growth in various body areas, selecting those most indicative of androgen excess to include into their hirsutism scoring system.
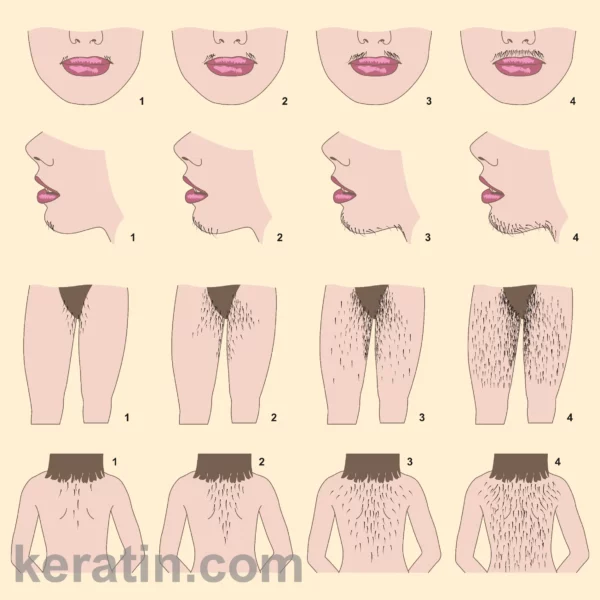
Originally, the Ferriman-Gallwey score included 11 body areas: upper lip, chin, chest, upper abdomen, lower abdomen, upper arms, lower arms, thighs, upper back, lower back, and buttocks. Each area was scored from 0 (no hair), through 1, 2, 3, to 4 (extensive hair growth), with the total score ranging from 0 to 44. However, subsequent studies refined the score by reducing the body areas to nine, excluding the forearms and lower legs due to their minimal contribution to the overall hirsutism assessment.
Methodology of the Ferriman-Gallwey Score: The revised Ferriman-Gallwey score assesses hair growth in the following nine body areas:
Upper lip
Chin
Chest
Upper abdomen
Lower abdomen
Upper back
Lower back
Upper arms
Thighs
Each area is scored from 0 to 4, based on the density and distribution of terminal hair:
0: No visible terminal hair
1: Minimal terminal hair
2: Moderate terminal hair
3: Extensive terminal hair, covering a large area
4: Severe terminal hair, densely covering the area
The scores for each area are summed to yield a total score, with a maximum possible score of 36 with the simplified 9 area scoring system. A score of 8 or higher is generally considered indicative of hirsutism, though this threshold may vary based on ethnic and racial differences in hair growth patterns.
Clinical Relevance of the Ferriman-Gallwey Score: The Ferriman-Gallwey score is a valuable tool in the clinical assessment of hirsutism for several reasons:
Diagnosis: The FG score helps diagnose hirsutism by providing a quantitative measure of hair growth. A score of 8 or higher suggests hirsutism, prompting further investigation into underlying causes such as polycystic ovary syndrome (PCOS), adrenal hyperplasia, androgen-secreting tumors, or some other candidate diagnosis.
Treatment Planning: The severity of hirsutism, as determined by the FG score, guides treatment decisions. Mild hirsutism (score 8-15) may be managed with cosmetic treatments and lifestyle changes, while moderate to severe hirsutism (score >15) often requires pharmacological interventions such as anti-androgens, oral contraceptives, insulin sensitizers, and similar.
Monitoring Treatment Efficacy: The FG score is useful for monitoring the effectiveness of treatment. Regular scoring allows clinicians to assess the reduction in hair growth over time and make necessary adjustments to the therapeutic regimen.
Research and Epidemiology: The FG score provides a standardized method for studying hirsutism in research and epidemiological studies, facilitating comparisons across different populations and treatment modalities.
Limitations of the Ferriman-Gallwey Score: Despite its widespread use, the Ferriman-Gallwey score has several limitations:
Subjectivity: The scoring relies on visual assessment, introducing subjectivity and potential inter-observer variability. Training and prior experience of the clinician doing the evaluations play a crucial role in ensuring consistent scoring.
Ethnic and Racial Variations: The FG score does not account for ethnic and racial differences in hair growth patterns. Women of Mediterranean, Middle Eastern, and South Asian descent tend to have higher baseline scores, which may lead to overestimation of hirsutism severity. Conversely, women of East Asian or Native American descent may have lower scores, potentially underestimating the condition.
Psychological Impact: The focus on hair growth patterns may not fully capture the psychological distress experienced by women with hirsutism. Comprehensive assessment should include evaluation of the impact on quality of life and mental health.
Non-Androgenic Hair Growth: The FG score primarily assesses androgen-dependent hair growth, potentially overlooking other causes of excessive hair growth, such as hypertrichosis or iatrogenic hair growth from medications.
Enhancing the Ferriman-Gallwey Score: To address these limitations, several modifications and complementary approaches have been proposed:
Training and Standardization: Implementing standardized training programs for clinicians can reduce inter-observer variability and improve the reliability of scoring.
Ethnicity-Specific Norms: Developing ethnicity-specific reference ranges can enhance the accuracy of hirsutism assessment in diverse populations, reducing the risk of misclassification.
Quality of Life Assessment: The FG score is an objective scoring system and takes no account of the individual affected. Incorporating quality of life measures, such as the Dermatology Life Quality Index (DLQI), alongside the FG score could provide a more holistic understanding of the impact of hirsutism on patients.
Technological Advances: Digital imaging and automated hair counting technologies offer potential for more objective and reproducible assessments of hair growth. These tools can complement the FG score, providing additional data for accurate diagnosis and monitoring. At this time there is no widely available automated assessment computer system available, but it’s probably coming soon.
Modifications to the Ferriman-Gallwey Score: Modifications of the Ferriman-Gallwey (FG) scoring method for hirsutism have aimed to enhance its diagnostic accuracy and applicability across different populations. Derksen and colleagues conducted a study involving 81 healthy female volunteers and 71 hirsute patients of childbearing age and Dutch ancestry, assessing 12 body regions, including all 11 areas originally surveyed by FG, plus the sideburns. Each area was scored from 0 to 4 based on the amount of terminal hair growth. They found that the scores for the upper lip, chin, lower abdomen, and thighs were most effective in distinguishing between normal and hirsute women, with a score of 6 or greater indicating hirsutism in all hirsute women and none in the controls. Yang and colleagues evaluated pregnant women and women with polycystic ovary syndrome in China. They concluded the greatest contribution to identifying hirsutism (defined as an modified FG score ≥5) could be limited to observation of new terminal hair growth on the upper lip, lower back, lower abdomen, and thigh. More recent modifications included assessing 12 body areas graded from 0 to 4, covering the nine areas described above plus the sideburns, lower jaw, upper neck (separate from the chin), and perineum. These adjustments aim to improve the score’s sensitivity and specificity for diverse populations.
Conclusion: The Ferriman-Gallwey score remains an essential tool in the clinical evaluation of hirsutism, offering a standardized method to quantify hair growth and guide diagnosis and treatment. While the score has limitations, ongoing efforts to enhance its accuracy and reliability, alongside complementary approaches, can improve the management of hirsutism. By considering ethnic variations, incorporating quality of life assessments, and leveraging technological advancements, clinicians can provide more comprehensive care for women with this challenging condition.
Garn SM. Types and distribution of the hair in man. Ann N Y Acad Sci. 1951 Mar;53(3):498–507.
1.
Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women. J Clin Endocrinol Metab. 1961 Nov;21:1440–7.
1.
Hatch R, Rosenfield RL, Kim MH, Tredway D. Hirsutism: implications, etiology, and management. Am J Obstet Gynecol. 1981 Aug 1;140(7):815–30.
1.
Derksen J, Moolenaar AJ, Van Seters AP, Kock DF. Semiquantitative assessment of hirsutism in Dutch women. Br J Dermatol. 1993 Mar;128(3):259–63.
1.
Barth JH. How robust is the methodology for trials of therapy in hirsute women? Clin Endocrinol (Oxf). 1996 Oct;45(4):379–80.
1.
Practice Committee of the American Society for Reproductive Medicine. The evaluation and treatment of androgen excess. Fertil Steril. 2006 Nov;86(5 Suppl 1):S241-247.
1.
Yildiz BO, Bolour S, Woods K, Moore A, Azziz R. Visually scoring hirsutism. Hum Reprod Update. 2010;16(1):51–64.
1.
Cook H, Brennan K, Azziz R. Reanalyzing the modified Ferriman-Gallwey score: is there a simpler method for assessing the extent of hirsutism? Fertil Steril. 2011 Nov;96(5):1266-1270.e1.
1.
Yang Y, Han Y, Wang W, Du T, Li Y, Zhang J, et al. Assessing new terminal body and facial hair growth during pregnancy: toward developing a simplified visual scoring system for hirsutism. Fertil Steril. 2016 Feb;105(2):494–500.
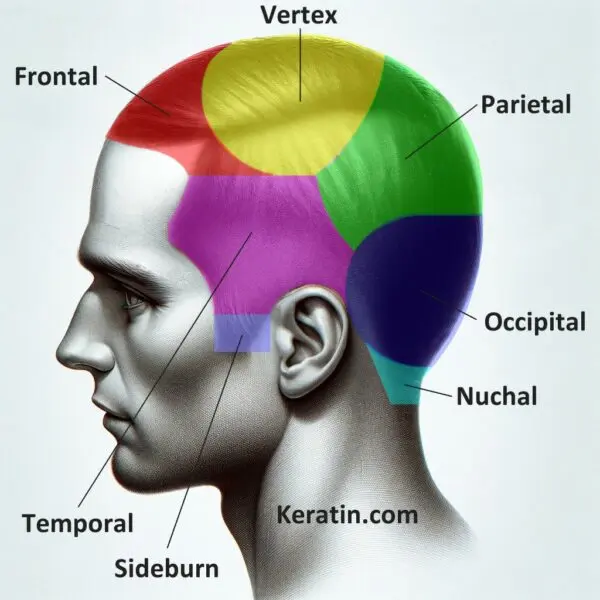
The human scalp is a complex and vital area of the body, especially when considering hair and skin health. For healthcare professionals, particularly those specializing…
When it comes to evaluating hair loss, one of the simplest clinical procedures a dermatologist may use is the hair pull test. Despite its straightforward…
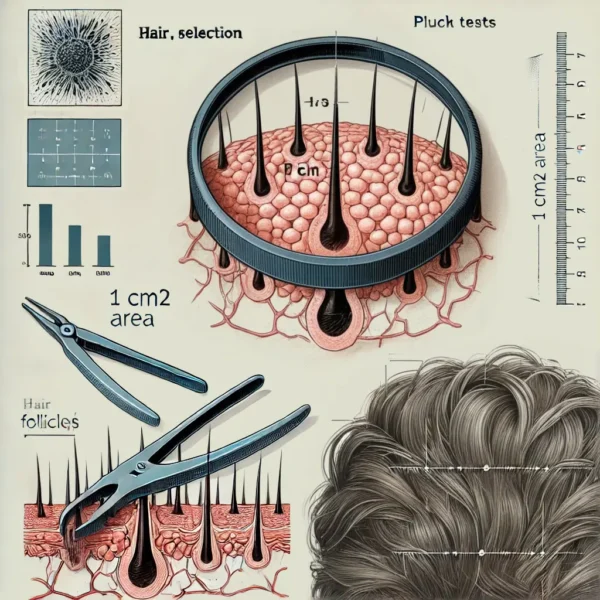
Hair analysis serves as a critical tool in both clinical and research settings, enabling scientists, dermatologists, and other medical professionals to assess hair growth patterns,…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.