Introduction: Anagen effluvium is a type of hair loss that occurs during the anagen growth phase of the hair cycle. Unlike other forms of hair loss such as telogen effluvium, where shedding occurs during the resting phase of the hair cycle, anagen effluvium is characterized by abrupt and rapid hair loss. This condition can have significant psychological and social impact due to its often sudden onset and the extent of hair loss that occurs. This article summarizes the etiology, pathophysiology, clinical presentation, and general management of anagen effluvium.
Etiology: Anagen effluvium is primarily caused by factors that disrupt the mitotic activity of hair follicle cells during the anagen hair growth phase. The most common cause of anagen effluvium is chemotherapy, where drugs target rapidly dividing cells, including those in hair follicles. Other causes include radiation therapy, exposure to toxic chemicals, and certain medications. Additionally, less common causes such as autoimmune diseases, severe infections, and systemic illnesses can also sometimes lead to development of anagen effluvium.
Chemotherapy : Chemotherapeutic agents such as cyclophosphamide, doxorubicin, and paclitaxel are well-documented causes of anagen effluvium. These drugs interfere with the DNA synthesis of rapidly dividing cells. Cancer cells are rapidly dividing cells, but so are hair follicle matrix cells as they make the hair fiber. The cells are blocked from proliferating leading to hair follicle dystrophy and subsequent hair loss.Radiation Therapy : Radiation, particularly when directed at the head and scalp, can induce anagen effluvium by damaging the DNA of cells in the skin and hair follicle cells.Toxic Chemicals : Exposure to heavy metals like thallium and arsenic, as well as other toxic agents, can disrupt hair follicle function, leading to hair loss. Again, the effects essentially prevent the hair fiber producing cells from growing.Medications : Certain medications, including antimitotic drugs and immunosuppressants, have also been implicated in causing anagen effluvium.Autoimmune Diseases : Conditions such as alopecia areata can occasionally manifest as anagen effluvium when the immune system mistakenly attacks the hair follicles. Usually, alopecia areata develops over time, and hair follicles are pushed into a telogen state. However, for a few people the development occurs very quickly. In these cases, the sudden hair follicle inflammation stops hair growth mid-stream and the hair sheds as an anagen effluvium. Pathophysiology: The pathophysiology of anagen effluvium involves the interruption of the anagen phase of the hair cycle. During the anagen phase, hair follicles are in a state of rapid growth, with high mitotic cell activity as the hair fiber is made. Disruption of this phase, whether through chemotherapeutic agents, radiation, or other factors, leads to apoptosis of the hair matrix cells. This results in the premature termination of hair growth and the subsequent shedding of hairs that were in the growth phase.
At the cellular level, the damage induced by chemotherapeutic agents or radiation therapy causes DNA damage and cell cycle arrest in the hair matrix cells. The hair follicles then enter a dystrophic anagen state, and/or a premature catagen-like state, leading to hair shedding. This process can be observed histologically by the presence of dystrophic anagen hairs, characterized by tapered or fractured hair shafts.
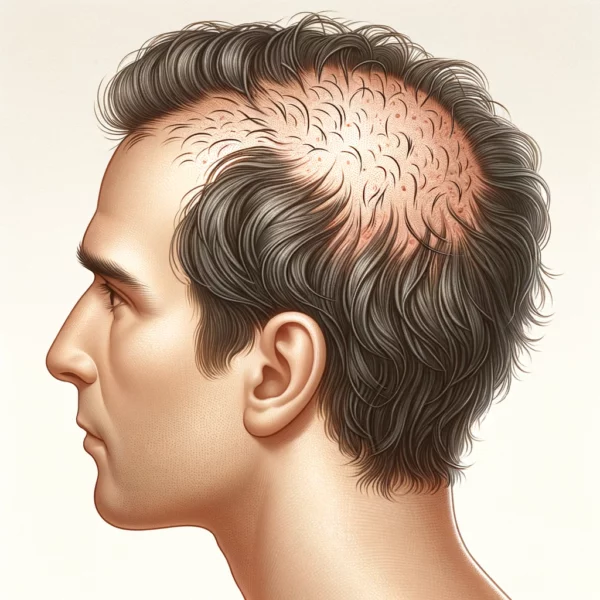
Clinical Presentation: Patients with anagen effluvium typically present with rapid and diffuse hair loss. The onset of hair loss is often within days to a few weeks of exposure to the causative agent, such as chemotherapy. Unlike other forms of hair loss that may progress gradually, anagen effluvium leads to a noticeable reduction in hair density over a short period.
The hair loss is usually non-scarring, meaning the hair follicles remain intact and capable of regrowth once the causative factor is removed or mitigated. In severe cases, patients may experience complete alopecia, including the loss of eyebrows, eyelashes, and body hair. For a few people, the hair does not grow back completely, or sometimes has changes in appearance (see below).
Diagnosis: The diagnosis of anagen effluvium is primarily clinical, based on the history of exposure to known causative agents and the characteristic pattern of hair loss. Examination of shed hair under a microscope can aid in the diagnosis by revealing specific features such as tapered hair shafts and the absence of visible telogen club hairs, which are indicative of anagen hair shedding.
Very occasionally, a scalp biopsy may be performed to differentiate anagen effluvium from other forms of hair loss – particularly when the shedding is diffuse and needs to be distinguished from other diffuse forms of hair loss such as diffuse alopecia areata, or telogen effluvium. Histopathological examination of the biopsy specimen typically shows dystrophic anagen hairs with tapered or fractured shafts, along with increased apoptosis of hair matrix cells.
Management and Treatment: The management of anagen effluvium primarily focuses on addressing the underlying cause and providing supportive care to the patient.
Chemotherapy-Induced Anagen Effluvium : In cases where chemotherapy is the causative agent, strategies to minimize hair loss include scalp cooling (cryotherapy), which can reduce the uptake of chemotherapeutic agents by hair follicle cells. The use of scalp cooling caps during chemotherapy sessions has shown some efficacy in reducing hair loss.Radiation Therapy : For patients undergoing radiation therapy, shielding the scalp or adjusting the radiation dose can help minimize hair loss. However, these measures may not always be feasible depending on the treatment requirements.Medications and Toxic Chemicals : Discontinuation or substitution of the offending medication, where possible, can lead to the cessation of hair loss and the initiation of regrowth. In cases of toxic chemical exposure, removal from the source of toxicity is crucial.Supportive Care : Topical minoxidil has been used off-label to promote hair regrowth in patients with anagen effluvium. While evidence of its efficacy is limited, in theory it may help accelerate the regrowth process.Cosmetic Solutions : Patients may benefit from cosmetic solutions such as wigs, hairpieces, and scalp camouflage products to manage the psychological and social impact of hair loss.Psychological Support : Given the potential psychological impact of sudden and severe hair loss, providing psychological support and counselling is an important aspect of the management plan. Prognosis: The prognosis for patients with anagen effluvium is generally favorable, particularly when the causative factor can be identified and addressed. Hair regrowth typically begins within weeks to months after the removal of the causative agent. However, the extent and rate of regrowth can vary among individuals and for some people it can take up to a year before hair follicles fully recover and start growing new hair.
In most cases, the hair that regrows is of normal thickness and texture. However, some patients may experience changes in hair color or texture during the initial regrowth phase. Persistent or incomplete regrowth is rare but can occur, especially in cases of prolonged or high-dose exposure to chemotherapeutic agents or radiation.
While it is not clear why some people have changes to the properties of their hair, or have incomplete hair regrowth, it’s assumed that the anagen effluvium inducing agent has probably affected the hair follicle stem cells in some way. Hair follicles contain epithelial stem cells that ultimately provide cells for hair fiber manufacture, mesenchymal stem cells that control size and shape of hair follicles, and melanocyte stem cells that control hair color. Chemicals and other agents that interfere with one or more of these stem cell populations could permanently alter hair growth parameters.
Conclusion: Anagen effluvium is a distinct form of hair loss characterized by the rapid shedding of hairs during the anagen phase of the hair cycle. Its etiology is diverse, with chemotherapy being the most common cause. Understanding the pathophysiology, clinical presentation, and management options is essential for healthcare providers to effectively diagnose and support patients experiencing this condition. With appropriate intervention and supportive care, most patients can expect to see a return to normal hair growth and regain their confidence and quality of life.
Bibliography
11711645 {11711645:S4PTQVPS},{11711645:ZCJAC5HB},{11711645:VF7NRQ6A},{11711645:URRDUB2N},{11711645:5CI8WGFM},{11711645:73MP42UT},{11711645:9634IQ57},{11711645:HCXDHQ5I},{11711645:V7VQD23E},{11711645:GRBK2F6R},{11711645:AWFTVFF2},{11711645:KQPXASKW} 1 vancouver 50 date asc 1525 https://www.keratin.com/wp-content/plugins/zotpress/ %7B%22status%22%3A%22success%22%2C%22updateneeded%22%3Afalse%2C%22instance%22%3Afalse%2C%22meta%22%3A%7B%22request_last%22%3A0%2C%22request_next%22%3A0%2C%22used_cache%22%3Atrue%7D%2C%22data%22%3A%5B%7B%22key%22%3A%229634IQ57%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Peter%20et%20al.%22%2C%22parsedDate%22%3A%221994-05%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BPeter%20RU%2C%20Braun-Falco%20O%2C%20Birioukov%20A%2C%20Hacker%20N%2C%20Kerscher%20M%2C%20Peterseim%20U%2C%20et%20al.%20Chronic%20cutaneous%20damage%20after%20accidental%20exposure%20to%20ionizing%20radiation%3A%20the%20Chernobyl%20experience.%20J%20Am%20Acad%20Dermatol.%201994%20May%3B30%285%20Pt%201%29%3A719%26%23x2013%3B23.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Chronic%20cutaneous%20damage%20after%20accidental%20exposure%20to%20ionizing%20radiation%3A%20the%20Chernobyl%20experience%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22R.%20U.%22%2C%22lastName%22%3A%22Peter%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22O.%22%2C%22lastName%22%3A%22Braun-Falco%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%22%2C%22lastName%22%3A%22Birioukov%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22N.%22%2C%22lastName%22%3A%22Hacker%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%22%2C%22lastName%22%3A%22Kerscher%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22U.%22%2C%22lastName%22%3A%22Peterseim%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22T.%22%2C%22lastName%22%3A%22Ruzicka%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22B.%22%2C%22lastName%22%3A%22Konz%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22G.%22%2C%22lastName%22%3A%22Plewig%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20The%20hazards%20of%20acute%20radiation%20exposure%20are%20well%20known.%20Bone%20marrow%20failure%20from%20total%20body%20gamma%20or%20neutron%20irradiation%20is%20the%20most%20clinically%20relevant%20aspect%20of%20acute%20radiation%20disease.%20With%20nonhomogeneous%20exposure%2C%20as%20is%20characteristic%20in%20accidents%2C%20other%20organ%20systems%2C%20such%20as%20the%20skin%2C%20may%20be%20more%20important%20in%20determining%20clinical%20prognosis.%20This%20became%20obvious%20in%20the%20two%20worst%20radiation%20accidents%20since%201945%2C%20the%20Chernobyl%20accident%20in%20April%201986%20and%20the%20Goiania%20accident%20in%20September%201987.%5CnOBJECTIVE%3A%20Our%20purpose%20was%20to%20describe%20the%20characteristic%20chronic%20sequelae%20of%20accidental%20cutaneous%20radiation%20in%20a%20group%20of%20patients%20who%20survived%20the%20Chernobyl%20nuclear%20power%20plant%20accident.%5CnMETHODS%3A%20Fifteen%20patients%20with%20the%20delayed%20type%20of%20the%20cutaneous%20radiation%20syndrome%20were%20examined%20between%20September%201991%20and%20January%201992.%20All%20patients%20had%20a%20history%20of%20acute%20radiation%20disease.%20The%20exposure%20pattern%20was%20characterized%20by%20partial%20body%20exposure%20with%20high%20doses%20of%20beta%20and%20gamma%20irradiation%20from%20radioactive%20water%2C%20steam%2C%20or%20dust.%5CnRESULTS%3A%20Radiation-induced%20lesions%20were%20confined%20primarily%20to%20the%20legs%20and%20distal%20arms%2C%20but%20sometimes%20involved%20up%20to%2050%25%20of%20the%20total%20body%20surface.%20In%20addition%20to%20telangiectases%2C%20radiation%20keratoses%2C%20and%20radiation%20ulcers%2C%20hemangiomas%2C%20hematolymphangiomas%2C%20splinter%20hemorrhages%20in%20the%20distal%20nail%20bed%2C%20lentiginous%20hyperpigmentation%2C%20and%20severe%20subcutaneous%20fibrosis%20were%20noted.%20No%20malignant%20transformation%20could%20be%20detected.%20Associated%20diseases%20included%20cataracts%2C%20chronic%20hepatitis%2C%20and%20recalcitrant%20bacterial%20and%20herpesvirus%20infections.%5CnCONCLUSION%3A%20After%20accidental%20partial%20body%20exposure%20to%20high%20doses%20of%20beta%20and%20gamma%20irradiation%2C%20the%20predominant%20involvement%20of%20the%20skin%2C%20described%20as%20the%20cutaneous%20radiation%20syndrome%2C%20can%20become%20the%20characteristic%20feature.%20This%20causes%20longlasting%2C%20serious%20diagnostic%20and%20therapeutic%20problems.%22%2C%22date%22%3A%221994-05%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fs0190-9622%2808%2981501-0%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220190-9622%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A50%3A18Z%22%7D%7D%2C%7B%22key%22%3A%2273MP42UT%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Paus%22%2C%22parsedDate%22%3A%221998-12%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BPaus%20R.%20Principles%20of%20hair%20cycle%20control.%20J%20Dermatol.%201998%20Dec%3B25%2812%29%3A793%26%23x2013%3B802.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Principles%20of%20hair%20cycle%20control%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22R.%22%2C%22lastName%22%3A%22Paus%22%7D%5D%2C%22abstractNote%22%3A%22The%20hair%20follicle%20%28HF%29%20undergoes%20life-long%20cyclic%20transformations%20between%20%26quot%3Bresting%26quot%3B%20%28telogen%29%2C%20growth%20%28anagen%29%2C%20and%20apoptosis-driven%20regression%20%28catagen%29.%20Contrary%20to%20conventional%20wisdom%2C%20cyclic%20remodelling%20affects%20even%20the%20distal%20HF%20epithelium%3B%20telogen%20is%20not%20a%20mere%20resting%20period%2C%20since%20it%20shows%20substantial%20metabolic%20and%20proliferative%20activity%20and%20may%20encompass%20a%20phase%20of%20controlled%20hair%20shaft-extrusion%20%28%26quot%3Bexogen%26quot%3B%29.%20Even%20under%20physiological%20circumstances%2C%20very%20few%20%28malfunctioning%3F%29%20HF%20may%20leave%20this%20cycle%20over%20time%20to%20be%20removed%20by%20inflammatory%20cells%20%28%26quot%3Bprogrammed%20organ%20deletion%26quot%3B%29.%20Although%20numerous%20systemic%2C%20metabolic%2C%20immunological%2C%20and%20nerve-derived%20factors%20%28e.g.%20hormones%2C%20cytokines%2C%20neuropeptides%2C%20neurotransmitters%2C%20mast%20cells%29%20can%20profoundly%20alter%20hair%20growth%20in%20vivo%2C%20neither%20vascular%20nor%20neural%20stimuli%20nor%20extrafollicular%20cells%20are%20essential%20for%20HF%20development%20or%20cycling.%20Rather%2C%20an%20intrafollicular%20%26quot%3Bhair%20cycle%20clock%26quot%3B%20of%20as%20yet%20unknown%20nature%20drives%20the%20HF%20cycle.%20This%20elusive%20chronobiological%20timing%20device%20likely%20exploits%20secondary%20changes%20in%20the%20intra-%20and%20perifollicular%20signalling%20milieu%20for%20guiding%20the%20HF%20through%20its%20transformations.%20However%2C%20the%20supreme%20generator%20of%20cycling%20activity%20%28%26quot%3Boscillator%26quot%3B%29%20that%20dictates%20any%20of%20these%20signalling%20switches%20is%20still%20as%20unknown%20as%20is%20its%20exact%20location.%20Since%2C%20clinically%2C%20the%20control%20of%20catagen%20is%20of%20paramount%20importance%20%28too%20early%20anagen%20termination%3A%20alopecia%2C%20effluvium%3B%20catagen%20too%20late%3A%20hirsutism%2C%20hypertrichosis%29%2C%20the%20controls%20of%20catagen-associated%20keratinocyte%20apoptosis%20and%20of%20dermal%20papilla%20secretory%20activities%20are%20discussed%20as%20crucial%20targets%20for%20future%20therapeutic%20manipulations.%22%2C%22date%22%3A%221998-12%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1346-8138.1998.tb02507.x%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220385-2407%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T14%3A03%3A37Z%22%7D%7D%2C%7B%22key%22%3A%22HCXDHQ5I%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Piraccini%20et%20al.%22%2C%22parsedDate%22%3A%222006-08%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BPiraccini%20BM%2C%20Iorizzo%20M%2C%20Rech%20G%2C%20Tosti%20A.%20Drug-induced%20hair%20disorders.%20Curr%20Drug%20Saf.%202006%20Aug%3B1%283%29%3A301%26%23x2013%3B5.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Drug-induced%20hair%20disorders%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Bianca%20Maria%22%2C%22lastName%22%3A%22Piraccini%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Matilde%22%2C%22lastName%22%3A%22Iorizzo%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Giulia%22%2C%22lastName%22%3A%22Rech%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Antonella%22%2C%22lastName%22%3A%22Tosti%22%7D%5D%2C%22abstractNote%22%3A%22Drugs%20may%20induce%20hair%20loss%2C%20stimulate%20hair%20growth%20or%2C%20more%20rarely%2C%20induce%20changes%20in%20the%20hair%20shape%20and%20colour.%20Drug-induced%20hair%20loss%20is%20usually%20completely%20reversible%20and%20is%2C%20in%20most%20cases%2C%20a%20consequence%20of%20a%20toxic%20effect%20of%20the%20drug%20on%20the%20hair%20follicle%20matrix.%20In%20rare%20cases%20alopecia%20may%20be%20permanent.%20Depending%20on%20type%20of%20drug%2C%20dosage%20and%20patient%20susceptibility%2C%20hair%20loss%20presents%20as%20telogen%20effluvium%2C%20anagen%20effluvium%20or%20both.%20Telogen%20effluvium%20is%20also%20commonly%20observed%20after%20discontinuation%20of%20drugs%20that%20prolong%20anagen%2C%20such%20as%20topical%20minoxidil%20and%20oral%20contraceptives.%20Although%20a%20large%20number%20of%20drugs%20have%20been%20occasionally%20reported%20to%20produce%20hair%20loss%2C%20only%20for%20a%20few%20drugs%20the%20relation%20between%20drug%20intake%20and%20hair%20loss%20has%20been%20proven.%22%2C%22date%22%3A%222006-08%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.2174%5C%2F157488606777934477%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221574-8863%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A57%3A56Z%22%7D%7D%2C%7B%22key%22%3A%22AWFTVFF2%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Tosti%20and%20Pazzaglia%22%2C%22parsedDate%22%3A%222007-04%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BTosti%20A%2C%20Pazzaglia%20M.%20Drug%20reactions%20affecting%20hair%3A%20diagnosis.%20Dermatol%20Clin.%202007%20Apr%3B25%282%29%3A223%26%23x2013%3B31%2C%20vii.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Drug%20reactions%20affecting%20hair%3A%20diagnosis%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Antonella%22%2C%22lastName%22%3A%22Tosti%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Massimiliano%22%2C%22lastName%22%3A%22Pazzaglia%22%7D%5D%2C%22abstractNote%22%3A%22Drugs%20may%20cause%20hair%20loss%2C%20stimulate%20hair%20growth%2C%20or%20induce%20changes%20in%20the%20hair%20shape%20and%20color.%20Drug-induced%20hair%20loss%20is%2C%20in%20most%20cases%2C%20a%20consequence%20of%20a%20toxic%20effect%20of%20the%20drug%20on%20the%20hair%20matrix.%20Although%20a%20large%20number%20of%20drugs%20have%20been%20occasionally%20reported%20to%20produce%20hair%20loss%2C%20the%20relationship%20between%20drug%20intake%20and%20hair%20loss%20has%20been%20proven%20only%20for%20a%20few%20agents.%20Type%20of%20hair%20loss%20%28telogen%20effluvium%2C%20anagen%20effluvium%2C%20or%20both%29%20depends%20on%20the%20drug%2C%20its%20dosage%2C%20and%20patient%26%23039%3Bs%20susceptibility.%20Drug-induced%20hair%20loss%20is%20usually%20reversible.%22%2C%22date%22%3A%222007-04%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.det.2007.01.005%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220733-8635%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A58%3A31Z%22%7D%7D%2C%7B%22key%22%3A%22KQPXASKW%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Tr%5Cu00fceb%22%2C%22parsedDate%22%3A%222009-03%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BTr%26%23xFC%3Beb%20RM.%20Chemotherapy-induced%20alopecia.%20Semin%20Cutan%20Med%20Surg.%202009%20Mar%3B28%281%29%3A11%26%23x2013%3B4.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Chemotherapy-induced%20alopecia%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ralph%20M.%22%2C%22lastName%22%3A%22Tr%5Cu00fceb%22%7D%5D%2C%22abstractNote%22%3A%22Few%20dermatologic%20conditions%20carry%20as%20much%20emotional%20distress%20as%20chemotherapy-induced%20alopecia%20%28CIA%29.%20The%20prerequisite%20for%20successful%20development%20of%20strategies%20for%20CIA%20prevention%20is%20the%20understanding%20of%20the%20pathobiology%20of%20CIA.%20The%20incidence%20and%20severity%20of%20CIA%20are%20variable%20and%20related%20to%20the%20particular%20chemotherapeutic%20protocol.%20CIA%20is%20traditionally%20categorized%20as%20acute%20diffuse%20hair%20loss%20caused%20by%20dystrophic%20anagen%20effluvium%3B%20however%2C%20CIA%20presents%20with%20different%20clinical%20patterns%20of%20hair%20loss.%20When%20an%20arrest%20of%20mitotic%20activity%20occurs%2C%20obviously%20numerous%20and%20interacting%20factors%20influence%20the%20shedding%20pattern.%20The%20major%20approach%20to%20minimize%20CIA%20is%20by%20scalp%20cooling.%20Unfortunately%2C%20most%20published%20data%20on%20scalp%20cooling%20are%20of%20poor%20quality.%20Several%20experimental%20approaches%20to%20the%20development%20of%20pharmacologic%20agents%20are%20under%20evaluation%20and%20include%20drug-specific%20antibodies%2C%20hair%20growth%20cycle%20modifiers%2C%20cytokines%20and%20growth%20factors%2C%20antioxidants%2C%20inhibitors%20of%20apoptosis%2C%20and%20cell-cycle%20and%20proliferation%20modifiers.%20Ultimately%2C%20the%20protection%20should%20be%20selective%20to%20the%20hair%20follicle%3B%20for%20example%2C%20topical%20application%2C%20such%20that%20the%20anticancer%20efficacy%20of%20chemotherapy%20is%20not%20hampered.%20Among%20the%20few%20agents%20that%20have%20been%20evaluated%20so%20far%20in%20humans%2C%20AS101%20and%20minoxidil%20were%20able%20to%20reduce%20the%20severity%20or%20shorten%20the%20duration%20of%20CIA%2C%20but%20could%20not%20prevent%20CIA.%22%2C%22date%22%3A%222009-03%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.sder.2008.12.001%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221558-0768%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T14%3A05%3A06Z%22%7D%7D%2C%7B%22key%22%3A%22URRDUB2N%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Kanwar%20and%20Narang%22%2C%22parsedDate%22%3A%222013%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BKanwar%20AJ%2C%20Narang%20T.%20Anagen%20effluvium.%20Indian%20J%20Dermatol%20Venereol%20Leprol.%202013%3B79%285%29%3A604%26%23x2013%3B12.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Anagen%20effluvium%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Amrinder%20J.%22%2C%22lastName%22%3A%22Kanwar%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Tarun%22%2C%22lastName%22%3A%22Narang%22%7D%5D%2C%22abstractNote%22%3A%22Disturbances%20of%20hair%20follicle%20cycling%20lie%20at%20the%20heart%20of%20most%20hair%20growth%20disorders%2C%20and%20have%20dramatic%20effects%20on%20visible%20hair%20growth%20and%20shedding.%20The%20two%20common%20disorders%20due%20to%20aberration%20in%20hair%20follicle%20cycling%20are%20telogen%20and%20anagen%20effluvium.%20Though%20a%20lot%20of%20literature%20addresses%20the%20problem%20of%20telogen%20effluvium%2C%20there%20are%20not%20many%20reviews%20on%20anagen%20effluvium%20or%20anagen%20hair%20loss.%20Anagen%20effluvium%20is%20considered%20synonymous%20with%20chemotherapy-induced%20alopecia%20and%20other%20causes%20are%20rarely%20considered.%20In%20this%20review%2C%20we%20try%20to%20discuss%20the%20etiopathogenesis%2C%20clinical%20presentation%2C%20differentials%2C%20and%20management%20issues%20in%20anagen%20effluvium.%20Anagen%20effluvium%20is%20the%20abrupt%20loss%20of%20hairs%20that%20are%20in%20their%20growing%20phase%20%28anagen%29%20due%20to%20an%20event%20that%20impairs%20the%20mitotic%20or%20metabolic%20activity%20of%20hair%20follicle.%20Chemotherapy%2C%20radiation%20and%20toxic%20chemicals%2C%20and%20sometimes%20inflammatory%20diseases%20like%20alopecia%20areata%20and%20pemphigus%20are%20also%20capable%20of%20diminishing%20the%20metabolic%20activity%20of%20hair%20follicles%20resulting%20in%20anagen%20hair%20loss.%20Although%20it%20is%20reversible%2C%20and%20hair%20regrowth%20occurs%20after%20a%20delay%20of%201-3%20months%3B%20sometimes%20it%20can%20lead%20to%20permanent%20alopecia%20and%20can%20be%20psychologically%20devastating%20with%20negative%20impact%20on%20individual%20perceptions%20of%20appearance%2C%20body%20image%2C%20sexuality%2C%20and%20self-esteem.%20For%20some%20patients%2C%20the%20emotional%20trauma%20may%20be%20so%20severe%20that%20it%20may%20lead%20to%20discontinuing%20or%20refusing%20therapy%20that%20might%20otherwise%20be%20beneficial.%20In%20such%20cases%2C%20a%20psychosomatic%20approach%20as%20well%20as%20empathic%20consideration%20of%20the%20patients%20concerns%20and%20fears%20as%20well%20as%20the%20provision%20of%20practical%20medical-aesthetic%20and%20styling%20tips%20are%20equally%20important%20and%20can%20be%20integrated%20in%20management.%22%2C%22date%22%3A%222013%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.4103%5C%2F0378-6323.116728%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%220973-3922%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A54%3A44Z%22%7D%7D%2C%7B%22key%22%3A%22ZCJAC5HB%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Freites-Martinez%20et%20al.%22%2C%22parsedDate%22%3A%222019-05%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BFreites-Martinez%20A%2C%20Shapiro%20J%2C%20Goldfarb%20S%2C%20Nangia%20J%2C%20Jimenez%20JJ%2C%20Paus%20R%2C%20et%20al.%20Hair%20disorders%20in%20patients%20with%20cancer.%20J%20Am%20Acad%20Dermatol.%202019%20May%3B80%285%29%3A1179%26%23x2013%3B96.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Hair%20disorders%20in%20patients%20with%20cancer%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Azael%22%2C%22lastName%22%3A%22Freites-Martinez%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jerry%22%2C%22lastName%22%3A%22Shapiro%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Shari%22%2C%22lastName%22%3A%22Goldfarb%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Julie%22%2C%22lastName%22%3A%22Nangia%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Joaquin%20J.%22%2C%22lastName%22%3A%22Jimenez%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ralf%22%2C%22lastName%22%3A%22Paus%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mario%20E.%22%2C%22lastName%22%3A%22Lacouture%22%7D%5D%2C%22abstractNote%22%3A%22Cytotoxic%20chemotherapies%2C%20molecularly%20targeted%20therapies%2C%20immunotherapies%2C%20radiotherapy%2C%20stem%20cell%20transplants%2C%20and%20endocrine%20therapies%20may%20lead%20to%20hair%20disorders%2C%20including%20alopecia%2C%20hirsutism%2C%20hypertrichosis%2C%20and%20pigmentary%20and%20textural%20hair%20changes.%20The%20mechanisms%20underlying%20these%20changes%20are%20varied%20and%20remain%20incompletely%20understood%2C%20hampering%20the%20development%20of%20preventive%20or%20therapeutic%20guidelines.%20The%20psychosocial%20impact%20of%20chemotherapy-induced%20alopecia%20has%20been%20well%20documented%20primarily%20in%20the%20oncology%20literature%3B%20however%2C%20the%20effect%20of%20other%20alterations%2C%20such%20as%20radiation-induced%20alopecia%2C%20hirsutism%2C%20and%20changes%20in%20hair%20color%20or%20texture%20on%20quality%20of%20life%20have%20not%20been%20described.%20This%20article%20reviews%20clinically%20significant%20therapy-related%20hair%20disorders%20in%20oncology%20patients%2C%20including%20the%20underlying%20pathophysiological%20mechanisms%2C%20severity%20grading%20scales%2C%20patient-reported%20quality%20of%20life%20questionnaires%2C%20management%20strategies%2C%20and%20future%20translational%20research%20opportunities.%22%2C%22date%22%3A%222019-05%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.jaad.2018.03.055%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221097-6787%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A56%3A31Z%22%7D%7D%2C%7B%22key%22%3A%225CI8WGFM%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Novice%20et%20al.%22%2C%22parsedDate%22%3A%222020-02%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BNovice%20T%2C%20Novice%20M%2C%20Shapiro%20J%2C%20Lo%20Sicco%20K.%20Chemotherapy-induced%20alopecia-A%20potentially%20preventable%20side%20effect%20with%20scalp%20cooling.%20J%20Am%20Acad%20Dermatol.%202020%20Feb%3B82%282%29%3Ae57%26%23x2013%3B9.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Chemotherapy-induced%20alopecia-A%20potentially%20preventable%20side%20effect%20with%20scalp%20cooling%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Taylor%22%2C%22lastName%22%3A%22Novice%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Madison%22%2C%22lastName%22%3A%22Novice%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jerry%22%2C%22lastName%22%3A%22Shapiro%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Kristen%22%2C%22lastName%22%3A%22Lo%20Sicco%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222020-02%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.jaad.2019.09.059%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221097-6787%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A56%3A55Z%22%7D%7D%2C%7B%22key%22%3A%22VF7NRQ6A%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Gupta%20et%20al.%22%2C%22parsedDate%22%3A%222021%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BGupta%20S%2C%20Khandpur%20S%2C%20Bhari%20N.%20Anagen%20Effluvium%3A%20A%20Trichoscopic%20Analysis.%20Indian%20Dermatol%20Online%20J.%202021%3B12%285%29%3A786%26%23x2013%3B7.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Anagen%20Effluvium%3A%20A%20Trichoscopic%20Analysis%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Savera%22%2C%22lastName%22%3A%22Gupta%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Sujay%22%2C%22lastName%22%3A%22Khandpur%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Neetu%22%2C%22lastName%22%3A%22Bhari%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222021%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.4103%5C%2Fidoj.IDOJ_18_20%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%222229-5178%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A56%3A01Z%22%7D%7D%2C%7B%22key%22%3A%22V7VQD23E%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Randolph%20and%20Tosti%22%2C%22parsedDate%22%3A%222021-03%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BRandolph%20M%2C%20Tosti%20A.%20Oral%20minoxidil%20treatment%20for%20hair%20loss%3A%20A%20review%20of%20efficacy%20and%20safety.%20J%20Am%20Acad%20Dermatol.%202021%20Mar%3B84%283%29%3A737%26%23x2013%3B46.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Oral%20minoxidil%20treatment%20for%20hair%20loss%3A%20A%20review%20of%20efficacy%20and%20safety%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Michael%22%2C%22lastName%22%3A%22Randolph%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Antonella%22%2C%22lastName%22%3A%22Tosti%22%7D%5D%2C%22abstractNote%22%3A%22BACKGROUND%3A%20Although%5Cu00a0topical%20minoxidil%20is%20an%20effective%20treatment%20option%20for%20hair%20loss%2C%20many%20patients%20are%20poorly%20compliant%20because%20of%20the%20necessity%20to%20apply%20the%20medication%20twice%20a%20day%2C%20undesirable%20hair%20texture%2C%20and%20scalp%20irritation.%5CnOBJECTIVE%3A%20In%20recent%20years%2C%20oral%20minoxidil%20at%20low%20dose%20has%20been%20proposed%20as%20a%20safe%20alternative.%20This%20study%20reviewed%20articles%20in%20which%20oral%20minoxidil%20was%20used%20to%20treat%20hair%20loss%20to%20determine%20its%20efficacy%20and%20safety%20as%20an%20alternative%20to%20topical%20minoxidil.%5CnMETHODS%3A%20PubMed%20searches%20were%20performed%20to%20identify%20articles%20discussing%20oral%20minoxidil%20as%20the%20primary%20form%20of%20treatment%20for%20hair%20loss%20published%20up%20to%20April%202020.%5CnRESULTS%3A%20A%20total%20of%2017%20studies%20with%20634%20patients%20were%20found%20discussing%20the%20use%20of%20oral%20minoxidil%20as%20the%20primary%20treatment%20modality%20for%20hair%20loss.%20Androgenetic%20alopecia%20was%20the%20most%20studied%20condition%2C%20but%20other%20conditions%20included%20telogen%20effluvium%2C%20lichen%20planopilaris%2C%20loose%20anagen%20hair%20syndrome%2C%20monilethrix%2C%20alopecia%20areata%2C%20and%20permanent%20chemotherapy-induced%20alopecia.%5CnLIMITATIONS%3A%20Larger%20randomized%20studies%20comparing%20the%20efficacy%5C%2Fsafety%20of%20different%20doses%20with%20standardized%20objective%20measurements%20will%20be%20needed%20to%20clarify%20the%20best%20treatment%20protocol.%5CnCONCLUSION%3A%20Oral%20minoxidil%20was%20found%20to%20be%20an%20effective%20and%20well-tolerated%20treatment%20alternative%20for%20healthy%20patients%20having%20difficulty%20with%20topical%20formulations.%22%2C%22date%22%3A%222021-03%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.jaad.2020.06.1009%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221097-6787%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T14%3A00%3A41Z%22%7D%7D%2C%7B%22key%22%3A%22GRBK2F6R%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Starace%20et%20al.%22%2C%22parsedDate%22%3A%222022-03%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BStarace%20M%2C%20Orlando%20G%2C%20Bruni%20F%2C%20Alessandrini%20A%2C%20Piraccini%20BM.%20Anagen%20effluvium%20and%20the%20role%20of%20trichoscopy.%20Clin%20Exp%20Dermatol.%202022%20Mar%3B47%283%29%3A589%26%23x2013%3B91.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Anagen%20effluvium%20and%20the%20role%20of%20trichoscopy%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%22%2C%22lastName%22%3A%22Starace%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22G.%22%2C%22lastName%22%3A%22Orlando%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22F.%22%2C%22lastName%22%3A%22Bruni%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%22%2C%22lastName%22%3A%22Alessandrini%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22B.%20M.%22%2C%22lastName%22%3A%22Piraccini%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222022-03%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1111%5C%2Fced.14982%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221365-2230%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A55%3A28Z%22%7D%7D%2C%7B%22key%22%3A%22S4PTQVPS%22%2C%22library%22%3A%7B%22id%22%3A11711645%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Alhanshali%20et%20al.%22%2C%22parsedDate%22%3A%222023-08%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%201.35%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BAlhanshali%20L%2C%20Buontempo%20M%2C%20Shapiro%20J%2C%20Lo%20Sicco%20K.%20Medication-induced%20hair%20loss%3A%20An%20update.%20J%20Am%20Acad%20Dermatol.%202023%20Aug%3B89%282S%29%3AS20%26%23x2013%3B8.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Medication-induced%20hair%20loss%3A%20An%20update%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Lina%22%2C%22lastName%22%3A%22Alhanshali%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Michael%22%2C%22lastName%22%3A%22Buontempo%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jerry%22%2C%22lastName%22%3A%22Shapiro%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Kristen%22%2C%22lastName%22%3A%22Lo%20Sicco%22%7D%5D%2C%22abstractNote%22%3A%22This%20article%20discusses%20drug-induced%20hair%20loss%2C%20which%20can%20occur%20with%20many%20drugs%20including%20cytotoxic%20agents%2C%5Cu00a0biologics%2C%20and%20immunomodulating%20agents%2C%20among%20others.%20It%20outlines%20the%20diagnosis%20and%20management%5Cu00a0of%20drug-induced%20alopecia%2C%20with%20a%20focus%20on%20recently%20implicated%20drugs.%22%2C%22date%22%3A%222023-08%22%2C%22section%22%3A%22%22%2C%22partNumber%22%3A%22%22%2C%22partTitle%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.jaad.2023.04.022%22%2C%22citationKey%22%3A%22%22%2C%22url%22%3A%22%22%2C%22PMID%22%3A%22%22%2C%22PMCID%22%3A%22%22%2C%22ISSN%22%3A%221097-6787%22%2C%22language%22%3A%22eng%22%2C%22collections%22%3A%5B%22MQG6VMGS%22%5D%2C%22dateModified%22%3A%222024-06-11T13%3A57%3A13Z%22%7D%7D%5D%7D 1.
Peter RU, Braun-Falco O, Birioukov A, Hacker N, Kerscher M, Peterseim U, et al. Chronic cutaneous damage after accidental exposure to ionizing radiation: the Chernobyl experience. J Am Acad Dermatol. 1994 May;30(5 Pt 1):719–23.
1.
Paus R. Principles of hair cycle control. J Dermatol. 1998 Dec;25(12):793–802.
1.
Piraccini BM, Iorizzo M, Rech G, Tosti A. Drug-induced hair disorders. Curr Drug Saf. 2006 Aug;1(3):301–5.
1.
Tosti A, Pazzaglia M. Drug reactions affecting hair: diagnosis. Dermatol Clin. 2007 Apr;25(2):223–31, vii.
1.
Trüeb RM. Chemotherapy-induced alopecia. Semin Cutan Med Surg. 2009 Mar;28(1):11–4.
1.
Kanwar AJ, Narang T. Anagen effluvium. Indian J Dermatol Venereol Leprol. 2013;79(5):604–12.
1.
Freites-Martinez A, Shapiro J, Goldfarb S, Nangia J, Jimenez JJ, Paus R, et al. Hair disorders in patients with cancer. J Am Acad Dermatol. 2019 May;80(5):1179–96.
1.
Novice T, Novice M, Shapiro J, Lo Sicco K. Chemotherapy-induced alopecia-A potentially preventable side effect with scalp cooling. J Am Acad Dermatol. 2020 Feb;82(2):e57–9.
1.
Gupta S, Khandpur S, Bhari N. Anagen Effluvium: A Trichoscopic Analysis. Indian Dermatol Online J. 2021;12(5):786–7.
1.
Randolph M, Tosti A. Oral minoxidil treatment for hair loss: A review of efficacy and safety. J Am Acad Dermatol. 2021 Mar;84(3):737–46.
1.
Starace M, Orlando G, Bruni F, Alessandrini A, Piraccini BM. Anagen effluvium and the role of trichoscopy. Clin Exp Dermatol. 2022 Mar;47(3):589–91.
1.
Alhanshali L, Buontempo M, Shapiro J, Lo Sicco K. Medication-induced hair loss: An update. J Am Acad Dermatol. 2023 Aug;89(2S):S20–8.