Loose Anagen Hair Syndrome (LAHS) is a relatively rare hair disorder predominantly affecting children, particularly females with light-colored hair. LAHS is characterized by hair that can be easily and painlessly pulled from the scalp, and it results from an abnormality in the hair growth cycle. This article provides an in-depth exploration of LAHS, covering its pathophysiology, clinical presentation, diagnosis, and management.
Pathophysiology: To understand LAHS, it is useful to first grasp the basics of the hair growth cycle, which consists of three main phases: anagen (growth phase), catagen (transitional phase), and telogen (resting phase). In a healthy scalp, approximately 85-90% of hairs are in the anagen growth phase at any given time. During this phase, in the vast majority of people, the hair is firmly anchored in the follicle by a structure called the inner root sheath.
In individuals with LAHS, the anchoring mechanism is defective. Specifically, the inner root sheath fails to properly adhere to the hair shaft, resulting in loosely anchored anagen hairs that can be easily dislodged. This abnormality is thought to be linked to a premature keratinization of the inner root sheath or a defect in the keratin proteins that form the anchoring structures.
Clinical Presentation: LAHS typically presents in early childhood, with parents often noticing that their child’s hair is unusually thin, does not grow long, and can be effortlessly pulled from the scalp. The syndrome primarily affects the occipital (back) and parietal (side) regions of the scalp, although it can involve the entire scalp. Despite the ease with which hairs are removed, children with LAHS generally do not experience any pain or discomfort.
The condition is rare, affecting no more than 2 people in every million each year. The condition is more common in girls than boys. Published reports often claim it is often associated with fine, blond, or light-brown hair – but these reports refer to Caucasian/white children. A few recent reports from the Middle East and Asia indicate loose anagen syndrome can also be seen in children with dark/black hair. Other reports from the USA indicate seeing loose anagen hair syndrome in multi-racial children with dark hair.
Although the syndrome usually reveals itself in early childhood, it often improves with age, and many individuals see a spontaneous resolution of symptoms during their adolescence.
Diagnosis: The diagnosis of LAHS is primarily clinical, supported by a detailed patient history and physical examination. Trichoscopy, a non-invasive imaging technique, is frequently employed to examine hair and scalp. Typical trichoscopic findings in LAHS include:
Loose Anagen Hairs: Hairs that lack the usual root sheaths and can be easily extracted.
Deformed Hair Roots: Anagen hairs with misshapen or ruffled cuticles.
A definitive diagnosis is often confirmed by a hair pull test, where a gentle traction on a small cluster of hairs results in the extraction of numerous anagen hairs. Microscopic examination of these hairs reveals anagen hair roots without the inner root sheath, confirming the diagnosis.
Histopathological examination of scalp biopsies can provide additional insights, but is generally reserved for atypical or ambiguous cases. In LAHS, biopsy specimens typically show an increased proportion of anagen hairs with abnormal root sheaths and keratinization.
Differential Diagnosis: Several other conditions can mimic LAHS, necessitating a careful differential diagnosis. These conditions include:
Alopecia Areata: An autoimmune disorder causing patchy hair loss, distinguishable by the presence of exclamation mark hairs and a positive pull test for telogen hairs.
Telogen Effluvium: A condition characterized by excessive shedding of telogen hairs, often following a stressful event or systemic illness.
Trichotillomania: A psychiatric disorder involving compulsive hair pulling, typically associated with irregular hair loss patterns and broken hairs of varying lengths.
Short Anagen Syndrome: Hair follicles go through a relatively brief growth phase before the hair is shed. Unlike Loose anagen syndrome, short anagen syndrome hairs are mostly telogen club hairs.
Genetic and Environmental Factors: The exact etiology of LAHS remains unclear, although genetic predisposition is suspected. Familial cases of LAHS suggest a potential autosomal dominant inheritance pattern with incomplete penetrance. Genetic studies have identified mutations in genes related to hair follicle development and keratinization, such as the K6HF gene, which encodes a hair follicle-specific type II keratin.
Environmental factors, such as exposure to certain chemicals or traumatic hair care practices, may exacerbate the condition. However, no definitive environmental triggers have been conclusively identified.
Management: There is no specific cure for LAHS, and management primarily focuses on supportive care and minimizing hair trauma. Recommendations for managing LAHS include:
Gentle Hair Care: Using mild shampoos, avoiding excessive brushing or combing, and refraining from using harsh hair treatments or heat styling tools.
Protective Hairstyles: Opting for loose hairstyles that do not place undue tension on the hair, such as braids or buns.
Regular Trimming: Keeping hair trimmed to reduce the appearance of thinness and prevent tangling.
Minoxidil: At least three research articles reporting cases of loose anangen hair syndrome indicated use of topical minoxidil to improve hair growth. There was some modest effect.
In most cases, the prognosis is favorable, with many children experiencing significant improvement or complete resolution of symptoms during adolescence. For persistent cases, consultation with a dermatologist or a trichologist can be beneficial.
Health Impact: LAHS is primarily a cosmetic concern, there are no known health issues directly linked to the condition. There are some reports of people with Noonan syndrome, Mazzanti syndrome, or Costello syndrome also having loose anagen syndrome. The reason for the link is not clear, but these conditions are genetic and result in significant developmental issues for the affected child. Consequently, It’s likely that the genes involved in these conditions are also involved in hair growth and anchoring the hair fiber.
Psychological Impact and Support: However, it can have psychological implications, particularly for children and adolescents. The noticeable hair thinning and inability to grow long hair can affect self-esteem and lead to social anxiety or embarrassment. Providing psychological support and counseling can be crucial in managing these aspects of the condition.
Parents and caregivers play a vital role in offering reassurance and fostering a positive self-image in affected children. Joining support groups or connecting with other families facing similar challenges can also provide valuable emotional support and practical advice.
Future Directions: Research into the molecular mechanisms underlying LAHS is ongoing (albeit rather sporadically), with the aim of identifying potential therapeutic targets. Advances in genetic and proteomic technologies hold promise for unraveling the complex interactions between genes, proteins, and environmental factors in hair disorders like LAHS.
Conclusion: Loose Anagen Hair Syndrome is a rare, non-scarring hair disorder primarily affecting young children, characterized by easily pluckable anagen hairs due to defective anchoring. While the condition often resolves spontaneously with age, management mostly focuses on gentle hair care practices and psychological support to mitigate the cosmetic and emotional impact. In the longer term, ongoing research into the genetic and molecular basis of LAHS may pave the way for innovative treatments, offering hope for affected individuals and their families.
Understanding and addressing the complexities of LAHS requires a multidisciplinary approach, encompassing dermatology, genetics, psychology, and patient support. By continuing to advance our knowledge of hair biology and disorder mechanisms, we can improve the diagnosis, management, and quality of life for those living with LAHS.
Restrepo I, Otberg N, McElwee K, Shapiro J. Two sisters, two different hair shaft abnormalities. Br J Dermatol. 2009 Aug;161(2):479–80.
1.
Cantatore-Francis JL, Orlow SJ. Practical guidelines for evaluation of loose anagen hair syndrome. Arch Dermatol. 2009 Oct;145(10):1123–8.
1.
Chandran NS, Oranje AP. Minoxidil 5% solution for topical treatment of loose anagen hair syndrome. Pediatr Dermatol. 2014;31(3):389–90.
1.
Swink SM, Castelo-Soccio L. Loose Anagen Syndrome: A Retrospective Chart Review of 37 Cases. Pediatr Dermatol. 2016 Sept;33(5):507–10.
1.
Cranwell WC, Sinclair R. Loose anagen hair syndrome: Treatment with systemic minoxidil characterised by marked hair colour change. Australas J Dermatol. 2018 Nov;59(4):e286–7.
1.
Leerunyakul K, Suchonwanit P. A Case of Loose Anagen Hair Syndrome in a Southeast Asian Boy. Case Rep Dermatol. 2019;11(2):204–8.
1.
Jerjen R, Koh WL, Sinclair R, Bhoyrul B. Low-dose oral minoxidil improves global hair density and length in children with loose anagen hair syndrome. Br J Dermatol. 2021 May;184(5):977–8.
1.
Al Dhafiri M, Alhumaidy M. Loose Anagen Hair Syndrome in a Saudi Girl. Dermatol Pract Concept. 2021 Oct;11(4):e2021071.
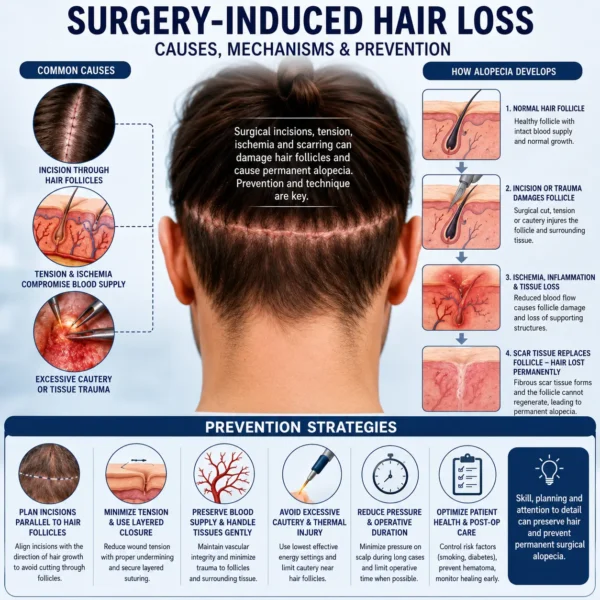
Hair loss after surgery is an under-recognized but clinically important complication. It may present as transient diffuse shedding or as permanent, localized alopecia confined to…
Trichotillomania (TTM), also known as hair-pulling disorder, is a relatively common condition that affects roughly 0.5% to 2.0% of the population. Despite being grouped with…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.