Trichotillomania, a condition characterized by the irresistible urge to pull out hair, is a complex disorder that involves a series of distinct yet interconnected behaviors and symptoms. These behaviors not only include the act of pulling hair but also the rituals preceding it, the method of pulling, the actions following the pulling, and the contextual circumstances. This article aims to delve into the various aspects of trichotillomania, from its triggers and manifestations to its unique signs like “flame hairs,” enhancing our understanding of this often misunderstood condition.
Certain rituals and behavioral patterns are often observed before the act of hair pulling occurs in trichotillomania. These events might include; running fingers through the hair, feeling the texture of individual strands, tugging at the hair, and visually inspecting the scalp and hairline in a mirror. The selection of hair for pulling may not be arbitrary but can be based on distinctive characteristics like length, color, texture, or its location on the hairline.
The technique used for hair removal varies from person to person in individuals with trichotillomania. Most frequently, people use their hands, especially their thumb and forefinger, to pull out their hair. However, some might also use tools like tweezers or other cosmetic devices for the same. It is usual to see one or two strands of hair being pulled out at a time, and several hairs can be removed during a single episode of pulling.
Actions performed after hair pulling are equally significant and seem quite unique to each individual. Some people may merely throw away the pulled hair, while others fiddle with the hair, examine it, might bite on it, or may even swallow some or all of it. Consuming hair can lead to the formation of hairballs, known as trichobezoars, which may potentially cause harm to the digestive tract. If this happens, there may be symptoms like abdominal discomfort, nausea, vomiting, and constipation. If not treated, trichobezoars can result in serious complications like bowel obstruction, intestinal bleeding, acute pancreatitis, obstructive jaundice, or a ruptured bowel which is a life threatening situation
There can also be environmental and emotional circumstances surrounding the act of hair pulling. Certain situations, such as watching television, reading, studying, or grooming in front of a mirror, can increase the tendency to pull hair for some people. Many individuals with trichotillomania report specific emotional states, such as stress or anxiety, a feeling of tension, or an urge to pull their hair, which precedes a pulling episode and is often relieved after the act of pulling.
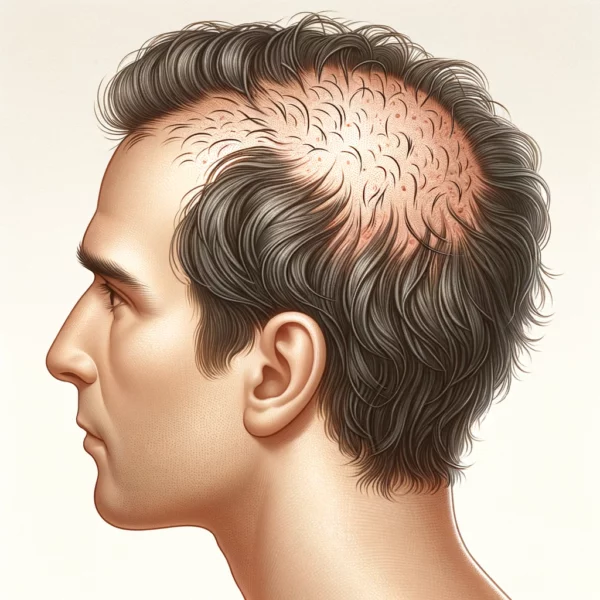
In clinical observations in the dermatology clinic, trichotillomania often shows as patchy alopecia with a diffuse or unusual shape, with patterns that may be irregular or non-scarring. It can appear as one or two patches, or it may involve the entire scalp diffusely. The patches of alopecia are unusually shaped, often with angular or irregular borders. At times, the hair loss in the crown area is encircled by a band of untouched hair at the edge, which can resemble the tonsures seen on Christian monks, a characteristic sometimes known (rather inappropriately) as the “Friar Tuck” sign.
The region of the scalp most frequently affected is the frontoparietal area, but eyebrows, upper eyelashes, and pubic area can also be areas of attention. Contrary to earlier beliefs that considered it relatively rare, pubic hair pulling is now recognized to be quite common among those suffering from trichotillomania. The face, limbs, underarms, and chest hair may be affected as well, though it’s less common to target these hair regions. Due to varied points of hair shaft breakage or repeated hair pulling, the lengths of the hair shafts can vary, leading to a coarse feeling when one touches the scalp.
As a result of the hair plucking in trichotillomania, the hair fibers can show some unusual features that can be best seen under the microscope or with a dermatoscope which is essentially a magnifying glass for looking closely at the skin and scalp. One feature that can be seen is “Flame hairs”; these were first described by Rakowska in 2014 as a trichoscopic sign of trichotillomania.
“Flame hairs” describe a particular characteristic of hair that has been repeatedly pulled. When a person with trichotillomania pulls their hair, it can cause the hair to break off unevenly, leaving behind a variety of hair lengths. Over time, this repeated pulling and breakage can cause damage to the hair shaft. Consequently, flame hairs are short, broken hairs that have a tapered or frayed end, giving an appearance somewhat like a flame, hence the term. The tapered end is a result of the hair being broken off, rather than cut cleanly as it would be with scissors.
This is one of several signs that dermatologists and other healthcare providers may look for when diagnosing trichotillomania. However, not all individuals with trichotillomania will have noticeable flame hairs, and the presence of flame hairs is not sufficient on its own to make a diagnosis. Diagnosis typically involves a comprehensive assessment, including a clinical interview and possibly psychological testing.
Understanding trichotillomania’s multifaceted nature, from the precursors to the act of pulling, the method of pulling, the post-pulling behaviors, and the emotional and environmental contexts, is critical for its effective diagnosis and treatment. Unique signs, such as “flame hairs,” provide additional diagnostic clues, even though their presence is not universal among all individuals with trichotillomania. While this condition presents unique challenges, a comprehensive understanding of its nuances can enable healthcare professionals to provide more effective and tailored interventions, offering hope and support to those grappling with this often hidden struggle.
Rakowska A, Slowinska M, Olszewska M, Rudnicka L. New trichoscopy findings in trichotillomania: flame hairs, V-sign, hook hairs, hair powder, tulip hairs. Acta Derm Venereol. 2014 May;94(3):303–6.
1.
Woods DW, Houghton DC. Diagnosis, evaluation, and management of trichotillomania. Psychiatr Clin North Am. 2014 Sept;37(3):301–17.
1.
Miteva M, Tosti A. Flame Hair. Skin Appendage Disord. 2015 Sept;1(2):105–9.
1.
Waśkiel A, Rakowska A, Sikora M, Olszewska M, Rudnicka L. Trichoscopy of alopecia areata: An update. J Dermatol. 2018 June;45(6):692–700.
1.
Martín JM, Montesinos E, Cordero P, Gonzalez V, Ramon D. Trichoscopy features of trichotillomania. Pediatr Dermatol. 2019 Mar;36(2):265–7.
1.
Kaczorowska A, Rudnicka L, Stefanato CM, Waskiel-Burnat A, Warszawik-Hendzel O, Olszewska M, et al. Diagnostic Accuracy of Trichoscopy in Trichotillomania: A Systematic Review. Acta Derm Venereol. 2021 Oct 7;101(10):adv00565.
A quiet form of hair loss: When people think of balding, they usually picture the familiar recessions and crowns of androgenetic alopecia (“male‑” or “female‑pattern”…
Introduction: An uneven hairline refers to a condition where the hairline lacks symmetry across the forehead or scalp, giving a visually unbalanced appearance. Hairlines naturally…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.