Introduction: Folliculitis denotes inflammation of the hair follicle’s superficial portion just below the skin surface. It often presents as erythematous papules, pustules or tender nodules around hair fibers. Whilst bacterial pathogens, particularly Staphylococcus aureus, are the predominant culprits in most folliculitis cases, fungal agents can also invade the follicular unit. Among these, species of the genus Candida represent an uncommon but clinically significant cause of folliculitis, particularly in individuals with predispositions such as immunosuppression, intravenous drug use, or who have systemic candidemia. Candida folliculitis can sometimes occur on the scalp and other body areas of hair, but more often develops around the groin. This article explores the anatomy of the pilosebaceous unit, the microbiology of Candida, the mechanisms by which it induces follicular inflammation, and current best practices for diagnosis, management and prevention of Candida folliculitis.
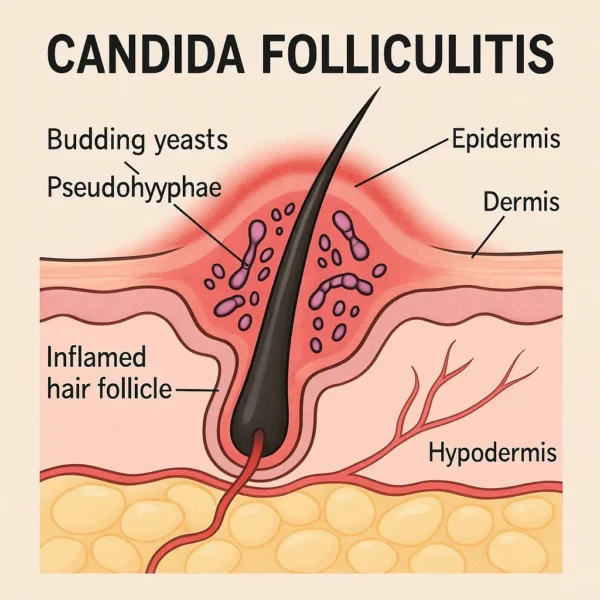
Anatomy of the Pilosebaceous Unit: Every human hair emerges from a complex pilosebaceous unit, which comprises three key segments:
Infundibulum: The most superficial region, extending from the follicular opening on the skin surface to the connection of the sebaceous gland duct; this area is rich in keratin and lipid secretions that fungal infections like to feed on.
Isthmus: The deeper mid-segment, located between the sebaceous duct and the attachment site of the arrector pili muscle; it houses stem cell niches that are crucial for follicular regeneration and hair growth cycling.
Inferior segment: Encompasses the hair bulb and dermal papilla; the site of active hair matrix cell proliferation and differentiation.
Inflammation confined to the infundibulum clinically manifests as folliculitis, whereas deeper involvement (e.g., of the isthmus or bulb) can lead to furuncles or cysts.
Microbiology of Candida Species: Candida spp. are opportunistic, unicellular yeasts that normally reside on skin and mucosal surfaces without causing disease. The most common human pathogen, Candida albicans, thrives in warm, moist environments, such as folds of skin, and can transition from a benign yeast form to an invasive, filamentous hyphal form under certain conditions. Other non-albicans species (e.g., C. glabrata, C. tropicalis) may also contribute to hair follicle infections, particularly in healthcare settings or in immunocompromised people.
Pathogenesis of Candida Folliculitis: Under normal conditions, skin-resident Candida are kept in check by mechanical barriers, sebum composition, resident bacterial flora, and host immune defenses (both innate and adaptive). Folliculitis arises when this equilibrium is disrupted, allowing fungal overgrowth and invasion of the follicular infundibulum. Key predisposing factors include:
Immunosuppression: HIV/AIDS, chemotherapy, corticosteroid therapy and diabetes mellitus impair neutrophil function and cell-mediated immunity in the body, this can enable fungal proliferation.
Intravenous drug use (IVDU): Contaminated injection equipment may introduce Candida directly into the bloodstream, leading to hematogenous seeding of follicles and disseminated candidiasis.
Prolonged antibiotic therapy: Broad-spectrum antibiotics disrupt the normal commensal bacterial populations, reducing competition which facilitates fungal overgrowth.
Occlusive clothing or tropical climates: Excess moisture and heat foster yeast proliferation within follicles. Hot weather and/or wearing hats etc. can encourage skin fungal overgrowth.
Once established in the hair follicle infundibulum, Candida elicits a mixed inflammatory response: neutrophils infiltrate the follicle, forming microabscesses (pustules), while macrophages and T lymphocytes orchestrate a more chronic granulomatous reaction in deeper infections.
Clinical Presentation: Patients with Candida folliculitis often report clusters of small, tender pustules or erythematous papules localized to hair-bearing areas (e.g., beard region, scalp, trunk or groin). Lesions may coalesce into nodules larger than 1 cm or develop crusted erosions upon rupture. Key distinguishing features of Candida folliculitis include:
Distribution: Pruritic or painful lesions in moist, intertriginous zones (e.g., arm pits, groin).
Systemic signs: Sometimes fever, chills or general malaise suggestive of candidemia in severe cases.
Association with candidemia: In IVDU or hospitalized patients with central venous catheters, pustular folliculitis may indicate invasive disease.
Refractoriness to antibacterial therapy: Lack of clinical response to antibiotics should prompt investigation for fungal etiology.
Differential diagnoses encompass bacterial folliculitis, pityrosporum (Malassezia) folliculitis, dermatophytic infections (tinea barbae), acneiform eruptions and noninfectious causes such as eosinophilic pustular folliculitis.
Diagnostic Approach: A systematic diagnostic work-up enhances accuracy and guides appropriate therapy:
Clinical assessment: Detailed history, including immunosuppressive conditions, medication use and IVDU. Physical examination noting lesion morphology, distribution and any signs of systemic involvement.
Microbiological studies: Potassium hydroxide (KOH) preparation: Scraping of pustular material may reveal budding yeasts and pseudohyphae under light microscopy. Fungal culture: Swabs or aspirates cultured on Sabouraud dextrose agar facilitate species identification and antifungal susceptibility testing. Blood cultures: Indicated if systemic signs are present, to rule out candidemia.
Histopathology (rarely required): Punch biopsy of a representative lesion can demonstrate neutrophilic infiltrates centered on the follicular infundibulum, with periodic acid–Schiff (PAS)-positive yeast and pseudohyphal elements.
Management Strategies: Therapeutic choices depend on infection severity, extent of skin involvement and host factors.
Topical antifungals: Azoles: Clotrimazole or ketoconazole cream applied twice daily for localized superficial infections. Ciclopirox: Broad-spectrum antifungal with anti-inflammatory properties.
Systemic antifungals: Fluconazole: typically given 150–200 mg orally once daily for 2–4 weeks; good bioavailability and favorable safety profile. Itraconazole: 200 mg orally once daily, often preferred for its broader spectrum and tissue penetration, especially in refractory cases. Echinocandins (e.g., caspofungin): Reserved for invasive candidiasis or fluconazole-resistant strains; administered intravenously under specialist guidance.
Adjunctive measures: Hygiene: Daily gentle cleansing with antifungal washes (e.g., chlorhexidine) and thorough drying of affected areas. Clothing: Loose-fitting garments and breathable fabrics to reduce moisture accumulation. Review of risk factors: Optimizing glycemic control in diabetics, minimizing systemic corticosteroid use where feasible, and addressing intravenous drug use.
Early initiation of systemic therapy is crucial when lesions are widespread, painful, or accompanied by systemic symptoms, to prevent progression to life-threatening invasive disease.
Monitoring and Prognosis: Most cases of superficial Candida folliculitis resolve completely with appropriate antifungal therapy, with clinical improvement often evident within 7–10 days. However, recurrences are not uncommon, particularly if predisposing conditions persist. Long-term management may necessitate:
Intermittent prophylactic antifungals: Low-dose fluconazole for patients with recurrent disease.
Addressing underlying immunosuppression: Collaboration with primary care or specialty teams to titrate immunomodulatory therapies; stringent glycemic control in diabetic patients.
Regular follow-up: Clinical assessment to ensure resolution and early detection of relapse or complications, such as scarring or secondary bacterial infection.
In cases of invasive candidiasis presenting with folliculitis, overall prognosis depends on prompt diagnosis, effective systemic antifungal therapy and management of central venous access devices or other sources of bloodstream infection.
Prevention: Preventive strategies focus on reducing follicular colonization and minimizing risk factors:
Skin care: Use of non-comedogenic moisturizers and avoidance of emollients in occluded areas. Regular application of antifungal sprays or powders in at-risk areas (e.g., between toes, groin).
Lifestyle modifications: Maintaining proper hygiene after sweating (e.g., showering post-exercise). Wearing breathable, moisture‐wicking fabrics. Avoiding shared personal care items (e.g., razors, towels).
Medical oversight: Judicious use of systemic antibiotics and corticosteroids. Monitoring patients on long-term immunosuppressants for early signs of fungal overgrowth.
Conclusion: Although Candida species are ubiquitous commensals, their invasion of hair follicles can culminate in significant morbidity, particularly in individuals with compromised immunity or other predisposing factors. Distinguishing Candida folliculitis from its bacterial and dermatophyte counterparts is essential, as misdiagnosis can lead to ineffective antibacterial therapy and disease progression. A thorough diagnostic work-up—including microscopy, culture and, where indicated, biopsy—combined with targeted antifungal treatment achieves favorable outcomes in most cases. Preventive measures and management of underlying risk factors are pivotal in reducing recurrence and safeguarding skin health. For clinicians and patients alike, heightened awareness of this uncommon yet impactful condition ensures timely intervention and optimal care.
Schirren C, Rieth H. [Folliculitis barbae caused by Candida albicans]. Arch Klin Exp Dermatol. 1956;202(6):577–89.
1.
Darcis JM, Etienne M, Demonty J, Christophe J, Pierard GE. Candida albicans septicemia with folliculitis in heroin addicts. Am J Dermatopathol. 1986 Dec;8(6):501–4.
1.
Dekio S, Imaoka C, Jidoi J. Candida folliculitis associated with hypothyroidism. Br J Dermatol. 1987 Nov;117(5):663–4.
1.
Süss K, Vennewald I, Seebacher C. Case report. Folliculitis barbae caused by Candida albicans. Mycoses. 1999;42(11–12):683–5.
1.
Kurita M, Kishimoto S, Kibe Y, Takenaka H, Yasuno H. Candida folliculitis mimicking tinea barbae. Acta Derm Venereol. 2000;80(2):153–4.
1.
Jalalat S, Hunter L, Yamazaki M, Head E, Kelly B. An outbreak of Candida albicans folliculitis masquerading as Malassezia folliculitis in a prison population. J Correct Health Care. 2014 Apr;20(2):154–62.
1.
Durdu M, Güran M, Kandemir H, Ilkit M, Seyedmousavi S. Clinical and Laboratory Features of Six Cases of Candida and Dermatophyte Folliculitis and a Review of Published Studies. Mycopathologia. 2016 Feb;181(1–2):97–105.
1.
Okwuwa I, Alam N, Wai R, Shayeb M, Sanchez A, Gandhi K, et al. Pubic Candida Folliculitis, A Case Report in a Patient With Recurrent Vaginal Candidiasis. J Family Reprod Health. 2023 Mar;17(1):62–4.
1.
Lijun Z, Lelai Y. Candida albicans Folliculitis and Preputial Balanitis. Mycopathologia. 2024 Sept 28;189(6):89.
Introduction: Folliculitis – the inflammation of hair follicles – most commonly arises from bacterial invasion, notably Staphylococcus aureus. However, a spectrum of viral agents can…
Introduction: Kerion Celsi is a severe, inflammatory form of tinea capitis, primarily affecting children. It is characterized by a boggy, purulent, and sometimes painful lesion…
Syphilis is a chronic, multistage infectious disease caused by the spirochete Treponema pallidum. Known historically as “the great imitator,” syphilis has puzzled clinicians for centuries…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.