Hair growth and its removal have sparked widespread interest, becoming a multi-billion-dollar industry. Society’s standard of beauty, particularly in the United States, often portrays bodies with an absence of hair as more feminine. With consumers on a relentless quest for the ideal hair removal solution, it’s critical to understand some key differences in hair growth conditions like hirsutism, hypertrichosis, and hyperandrogenism.
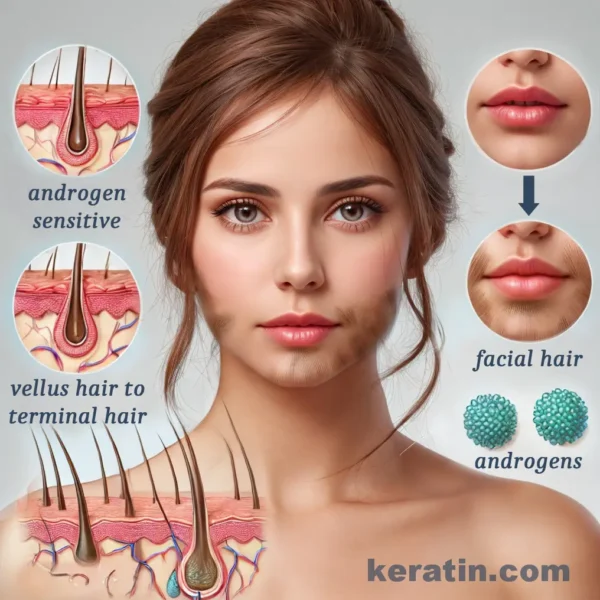
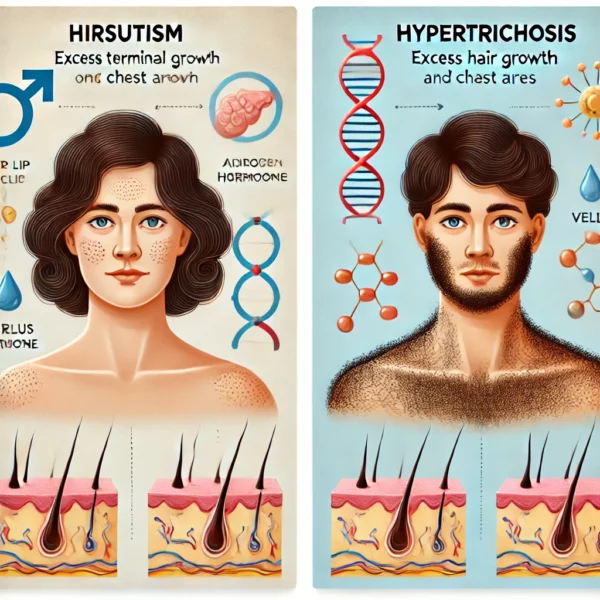
Understanding Hirsutism: Hirsutism is a condition characterized by the growth of excessive body or facial hair in women, mimicking the male pattern of hair growth. In general, the pattern of hair growth seen with hirsutism involves the production of pigmented terminal hair on the beard area of the face, the chest, lower abdomen, inner thighs and back. Often considered a “disease that needs to be treated” by many medical authorities, hirsutism can indicate an underlying disorder, which can usually be discerned via a medical history and blood tests.
The primary cause of hirsutism is the increased production, or skin sensitivity to, androgens commonly known as “male hormones.” Women with hirsutism can exhibit increased production of testosterone and androstenedione, though the increased level of hormone production can be quite subtle in many cases. For other women, hormonal levels can be essentially normal, rather, skin and hair follicles can be highly sensitive and responsive to androgen hormones. Hair follicles do have the ability to convert androgens locally in the skin making them into more potent hormones, such as dihydrotestosterone, that have a much greater effect on hair growth promotion.
Androgen disorders affect between 5% and 10% of all women, and the tendency towards hirsutism can often be inherited such that it runs in families. The prevalence of facial or body hair may increase with age, and while historically deemed taboo, 25% to 85% of middle-aged women remove unwanted hair. The percentage varies depending on which research journal articles you read – and probably reflects the different opinions on body hair beauty in different cultures and ethnicities.
Hypertrichosis Explained: While hirsutism refers to a male-like pattern of hair growth in women, hypertrichosis refers to excessive hair growth in regions not typically associated with a lot of hair, irrespective of gender. Hypertrichosis is comparative in nature, with a man with a particularly hairy chest or a woman with unusually hairy legs being diagnosed with the condition, as compared to others of the same sex, age, and ethnic background. This makes it quite hard to define hypertrichosis in consistent terms. What is normal hair growth for one group of people can be excessive hair growth for a different population. Sometimes, a dermatologist defers to the patient as they are the ultimate referees of what constitutes hypertrichosis for them.
It’s crucial to differentiate between hirsutism and hypertrichosis. Making this distinction will help to determine suitable treatment approaches. A woman with a beard would be diagnosed with hirsutism, not hypertrichosis, as women do not normally have beards. However, a woman with excessive hair on her calves would be described as hypertrichotic rather than hirsute. In more extreme examples, hypertrichosis may develop in skin that does not normally contain terminal hair follicles that produce pigmented hair fiber, such as on the cheeks and forehead, or even on the nose.
While some people may have quite extensive hypertrichosis, others can have hypertrichosis localised to just a small area of skin. This can occur due to changes in the skin just within the affected area. For example, a large mole can stimulate local hypertrichosis, a skin cancer may do the same, and even such things as constant rubbing of tight clothing can stimulate increased hair growth in the affected area.
Hyperandrogenism: While the diagnoses of hirsutism and hypertrichosis focus on hair growth patterns, hyperandrogenism describes a hormonal imbalance in women marked by significantly increased production of male hormones; with obvious changes in hormone concentration that are readily apparent with a blood test. This condition is often linked to a variety of causes, including chronic anovulation (i.e., polycystic ovarian syndrome; PCOS), congenital adrenal hyperplasia, ovarian tumors, adrenal gland problems, pregnancy-related issues, and certain drugs.
The most frequently observed clinical issue associated with hyperandrogenism is irregular menstrual cycles and the onset of hirsutism during the teens or early 20s. These are often symptoms of polycystic ovarian syndrome. Hair loss, acne, deepening of the voice, and sometimes increased muscle mass can also be symptoms of hyperandrogenism.
Bringing It All Together: It must be said that people have widely varying opinions on what’s considered excessive hair growth and attitudes vary depending on location across the world, ethnicity, culture, and religion. Plus these views can change over time (anyone remember the hairy 1970s?). In general however, North American, Western European, and far East Asian ideals of beauty focus on a relative lack of body hair in the 2020s. While hair removal is a key element of beauty standards in many societies, it’s vital to comprehend the medical underpinnings behind different patterns of hair growth. Understanding the distinctions between hirsutism, hypertrichosis, and hyperandrogenism helps in addressing potential underlying health issues and supports a more inclusive, diverse standard of beauty.
As science progresses, breaking the taboo around these conditions and acknowledging the commonality of such issues, particularly among middle-aged women, can pave the way for better education, understanding, and acceptance. Unwanted hair growth is not simply a cosmetic issue, but may also be a window into a person’s overall health, prompting necessary discussions and actions for proper medical attention and care.
Azziz R, Carmina E, Sawaya ME. Idiopathic hirsutism. Endocr Rev. 2000 Aug;21(4):347–62.
1.
Trüeb RM. Causes and management of hypertrichosis. Am J Clin Dermatol. 2002;3(9):617–27.
1.
Wendelin DS, Pope DN, Mallory SB. Hypertrichosis. J Am Acad Dermatol. 2003 Feb;48(2):161–79; quiz 180–1.
1.
Rosenfield RL. Hirsutism and the variable response of the pilosebaceous unit to androgen. J Investig Dermatol Symp Proc. 2005 Dec;10(3):205–8.
1.
Rosenfield RL. Clinical practice. Hirsutism. N Engl J Med. 2005 Dec 15;353(24):2578–88.
1.
Escobar-Morreale HF, Carmina E, Dewailly D, Gambineri A, Kelestimur F, Moghetti P, et al. Epidemiology, diagnosis and management of hirsutism: a consensus statement by the Androgen Excess and Polycystic Ovary Syndrome Society. Hum Reprod Update. 2012;18(2):146–70.
Introduction: Hyperandrogenis is, a condition characterized by the excessive production of androgens (male hormones) in women. It is a significant contributor to various clinical signs,…
Hair growth is a normal physiological process that varies widely among individuals based on genetic, hormonal, and environmental factors. However, certain conditions can lead to…
Wilgefortis, a figure more of folklore than religion, often surfaces in narratives marked by her distinguishing facial hair, leading to the colloquial moniker ‘The Bearded…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.