Male pattern hair loss is often diagnosed with the help of a classification system using diagrammatic representations of progressively more extensive hair loss. Originally designed by Hamilton in the 1950s, the pattern hair loss classification system was modified to its current form by Norwood in the 1970s. Norwood also added grades IIIa, III vertex, IVa and Va to Hamilton’s original classification scale.
There are now seven recognized categories of male androgenetic alopecia along with various subtypes based on Norwood’s classification system. Frequently when consulting with a dermatologist the diagnosis of androgenetic alopecia will be made in reference to the classification and you will be given your category such as “type III” or similar. These classification scales are used extensively in monitoring treatment trials.
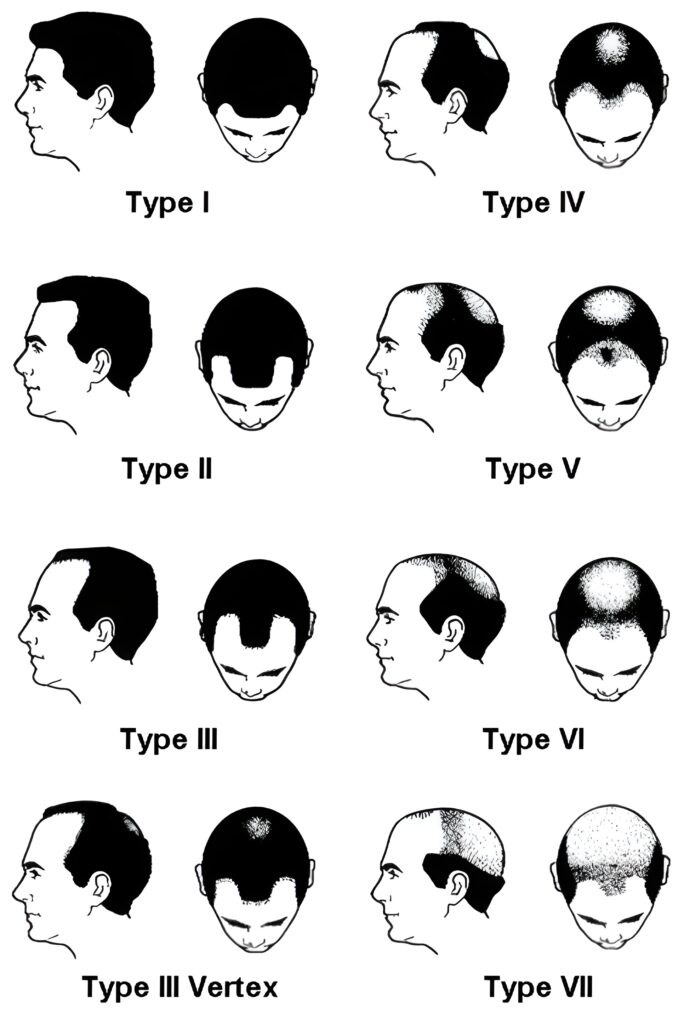
The Norwood male pattern hair loss scale: Norwood’s basic scale is illustrated and summarized below. Open the image in a new window for a larger picture.
Type I. Minimal or no recession of the hair line.
Type II. Triangular, usually symmetrical, areas of recession at the frontotemporal hair line.
Type III. This represents the minimal extent of hair loss sufficient to be considered as baldness according to Norwood. Most type III scalps have deep symmetrical recession at the temples that are bare or only sparsely covered by hair.
Type III vertex. In this presentation, the hair loss is primarily from the vertex with more limited recession of the frontotemporal hair line that does not exceed the degree of recession seen in type III.
Type IV. The frontotemporal recession is more severe than in type III. There is sparse hair or no hair on the vertex. The two areas of hair loss are seperated by a band of moderately dense hair that extends across the top of the scalp. This band connects with the fully haired fringe on the sides of the scalp. Type IV is distinguished from type III vertex in which the loss is primarily from the vertex.
Type V. The vertex hair loss region is still seperated from the frontotemporal region but it is less distinct. The band of hair across the crown is narrower and sparser. The vertex and frontotemporal regions of hair loss are bigger. Viewed from above, types V, VI, and VII are all characterized by surviving hair on the sides and back of the scalp forming a distinct horseshoe shape.
Type VI. The bridge of hair that crossed the crown is now gone with only sprase hair remaining. The frontotemporal and vertex regions are now joined together and the extent of hair loss is greater.
Type VII. The most severe form of hair loss presents as extensive loss. A narrow band of hair in a horseshoe shape survives on the sides and back of the scalp. This hair is usually not dense and may be quite fine. The hair is also sparse on the nape of the neck and in a semi circle over both ears.
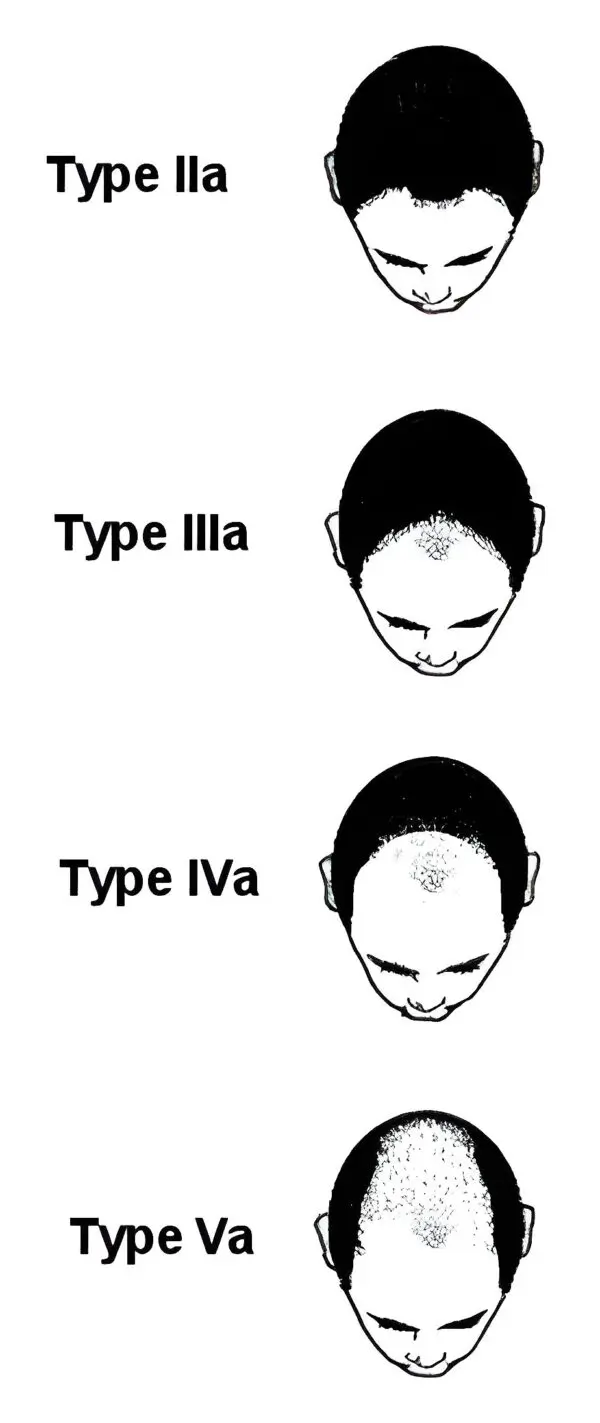
The Norwood male pattern baldness classification system type A variant: Norwood also defined a type A variant from his standard calssification system. He indicated that this variation in hair loss pattern affected up to 3% of the men in his studies. It is distinguished by two major features and two minor features.
The major features are: 1) the anterior border of the hairline progresses to the rear without leaving an island of hair in the mid frontal region. 2) There is no simultaneous development of a bald area on the vertex. Instead the frontal hair line recession keeps progessing to the rear of the scalp.
The minor features are; 1) There is a persistent sparse hair scattering in the area of hair loss. 2) The horseshoe shaped fringe areas of hair that remain on the side and back of the scalp tend to be wider and reach higher on the head comapred to Norwood’s standard classification.
Norwood OT. Hair Transplant Surgery. Thomas; 1973. 158 p.
1.
Norwood OT. Male pattern baldness: classification and incidence. South Med J. 1975 Nov;68(11):1359–65.
1.
Rhodes T, Girman CJ, Savin RC, Kaufman KD, Guo S, Lilly FR, et al. Prevalence of male pattern hair loss in 18-49 year old men. Dermatol Surg. 1998 Dec;24(12):1330–2.
1.
Hogan DJ, Chamberlain M. Male pattern baldness. South Med J. 2000 July;93(7):657–62.
1.
Ellis JA, Sinclair R, Harrap SB. Androgenetic alopecia: pathogenesis and potential for therapy. Expert Rev Mol Med. 2002 Nov 19;4(22):1–11.
Androgenetic alopecia (AGA), more commonly known as male pattern baldness, is a prevalent condition affecting a significant proportion of men across the globe. Characterized by…
Androgenetic alopecia (AGA) – most commonly referred to as male pattern hair loss – is the most frequent form of hair loss in adult men.…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.